Spread of Infection
| Home | | Pharmaceutical Microbiology | | Pharmaceutical Microbiology |Chapter: Pharmaceutical Microbiology : Vaccination And Immunization
Infectious diseases may either be spread from a common reservoir (common source) of the infectious agent that is distinct from the diseased individuals, or through a population by serial transfer from diseased to healthy, susceptible individuals .
SPREAD OF INFECTION
Infectious diseases may either be spread from a common reservoir (common source) of the infectious agent that is distinct from the diseased individuals, or through a population by serial transfer from diseased to healthy, susceptible individuals (propagated source; Figure 10.2).
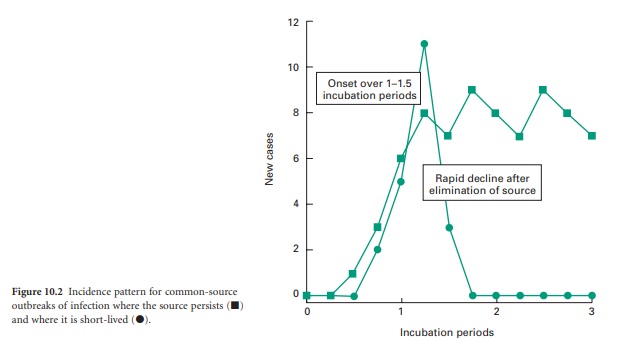
1) Common-Source Infections
In common source infections, potential reservoirs of infection include infected drinking-water, contaminated water vapour from a cooling tower, or contaminated food. In the simplest of cases the source of the infection is transient (i.e. food sourced to a single retail outlet, or to an isolated event such as a dinner party). In such instances, the onset of new cases will be phased over a timescale approximately equivalent to one incubation period, and the decline in new cases closely follows the elimination of the source (Figure 10.2). This leads to an acute outbreak of infection, limited to those linked with the source. Such incidents are epitomized by the 1996 outbreak of Escherichia coli O157 infections in Lanarkshire, Scotland, that resulted in 5 deaths and left 280 people ill. Similarly, in Clemenstone, South Wales, an outbreak resulted in 157 cases of E. coli including the death of a 5-year-old boy in 2005. Both of these outbreaks were linked to a single retail outlet.
If the source of the infection persists beyond the onset, then the incidence of new cases may be maintained at a level that is commensurate with the infectivity of the pathogen and the frequency of exposure of individuals. For those infectious diseases that are transmitted to humans via insect vectors that may act as reservoirs of infection, onset and decline phases of epidemics are rarely observed, other than as reflections of the seasonal variation in the prevalence of the insect. Diseases such as these are generally controlled by public health measures and environmental control of the insect vector with vaccination and immunization being deployed to protect individuals (e.g. yellow fever vaccination).
2) Propagated-Source Infections
Propagated outbreaks of infection relate to the direct transmission of an infective agent from a diseased individual to a healthy, susceptible one. Mechanisms of such transmission have been described in Chapter 7 and include inhalation of infective aerosols such as with measles, mumps and diphtheria; direct physical contact such as may occur with syphilis, herpesvirus and human papillomavirus; and, where sanitation standards are poor, through the introduction of infected faecal material into drinking-water (i.e. cholera and typhoid fever) or onto food (e.g. Salmonella and Campylobacter). The ease of transmission, and hence the rate of onset of an epidemic, relates to the susceptibility status and general state of health of the individuals concerned, the virulence properties of the organism, the route of transmission, the duration of the infective period associated with the disease, behavioural patterns, age of the population group and the population density (i.e. urban versus rural).
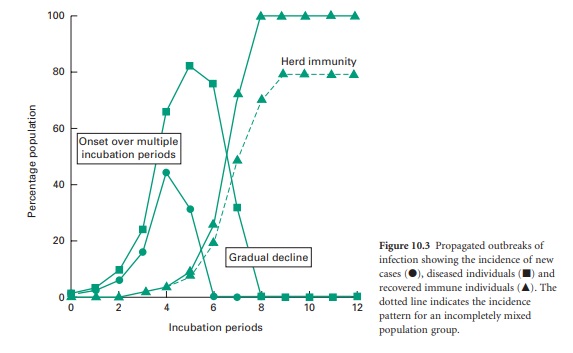
Each infectious individual will be capable of transmitting the disease to the susceptible individuals that they encounter during their infectious period. The number of persons to which a single infectious individual might transmit the disease and hence the rate of occurrence of the infection within the population will depend upon the population densities of susceptible and infective individuals, the degree and nature of their social interaction and the duration and timing of the infective period. If infectivity precedes the manifestation of disease, then spread of the infection may be greater than if these were concurrent. As each infected individual will in turn, become a source of infection, this leads to a near exponential increase in the incidence of disease. Figure 10.3 shows the incidence of disease within a population group. This group is perfectly mixed and all individuals are susceptible to the infection. The model infection has an incubation period of 1 day and an infective period of 2 days commencing at the onset of symptoms with recovery occurring 1 day later. For the sake of this illustration it has been assumed that each infective individual will infect two others per day until the entire population group has contracted the disease (solid lines). In reality, the rate of transmission will decrease as the epidemic progresses, because recovered individuals may become immune to further infection, reducing the population density of susceptible individuals, and thereby the likelihood of onward transmission. Epidemics therefore often cease before all members of the community have been infected (Figure 10.3, dotted line). If the proportion of immune individuals within a population group can be maintained above this threshold level then the likelihood of an epidemic arising from a single isolated infection incident is small (this is referred to as herd immunity). The threshold level itself is a function of the infectivity of the agent and the population density. Outbreaks of measles and chickenpox therefore tend to occur annually in the late summer among children attending school for the first time. This has the effect of concentrating all susceptible individuals in one, space and thereby reducing the proportion of immune subjects to a value below the threshold for propagated transmission. An effective vaccination programme that maintains the proportion of individuals who are immune to a given infectious disease above the critical threshold level for herd immunity. Such a programme will not prevent isolated cases of infection but will prevent these from becoming epidemic.
Related Topics
