Chapter Summary, Questions Answers - Phospholipid, Glycosphingolipid, and Eicosanoid Metabolism
| Home | | Biochemistry |Chapter: Biochemistry : Phospholipid, Glycosphingolipid, and Eicosanoid Metabolism
Phospholipids are polar, ionic compounds composed of an alcohol (for example, choline or ethanolamine) attached by a phosphodiester bond to either diacylglycerol (DAG), producing phosphatidylcholine or phosphatidylethanolamine, or to the amino alcohol sphingosine.
CHAPTER SUMMARY
Phospholipids are
polar, ionic compounds composed of an alcohol (for example, choline or
ethanolamine) attached by a phosphodiester bond to either diacylglycerol (DAG),
producing phosphatidylcholine or phosphatidylethanolamine, or to the amino
alcohol sphingosine (Figure 17.25 ). Addition of a long-chain fatty acid to
sphingosine produces a ceramide. Addition of a phosphorylcholine produces the
phospholipid sphingomyelin. Phospholipids are the predominant lipids of cell membranes.
Nonmembrane phospholipids serve as components of lung surfactant and bile. Dipalmitoylphosphatidylcholine,
also called dipalmitoyl lecithin, is the major lipid component of lung
surfactant. Insufficient surfactant production causes respiratory distress
syndrome. Phosphatidylinositol (PI) serves as a reservoir for arachidonic acid
in membranes. The phosphorylation of membrane-boundPI produces phosphatidylinositol
4,5-bisphosphate (PIP2). This compound is degraded by phospholipase C in
response to the binding of a variety of neurotransmitters, hormones, and growth
factors to membrane G protein–coupled receptors. The products of this
degradation, inositol 1,4,5-trisphosphate (IP3) and DAG mediate the
mobilization of intracellular calcium and the activation of protein kinase C,
which act synergistically to evoke cellular responses. Specific proteins can be
covalently attached via a carbohydrate bridge to membrane-bound
phosphatidylinositol (glycosyl phosphatidylinositol, or GPI), forming a GPI
anchor. A deficiency in the synthesis of GPI in hematopoietic cells results in
a hemolytic disease, paroxysmal nocturnal hemoglobinuria. The degradation of
phosphoglycerides is performed by phospholipases found in all tissues and
pancreatic juice. Sphingomyelin is degraded to a ceramide plus
phosphorylcholine by the lysosomal enzyme sphingomyelinase, a deficiency of
which causes Niemann-Pick (A + B) disease. Glycosphingolipids are derivatives
of ceramides to which carbohydrates have been attached. When one sugar molecule
is added to the ceramide, a cerebroside is produced. If an oligosaccharide is
added, a globoside is produced. If an acidic N-acetylneuraminic acid molecule
is added, a ganglioside is produced. Glycosphingolipids are found predominantly
in cell membranes of the brain and peripheral nervous tissue, with high
concentrations in the myelin sheath. They are antigenic. Glycolipids are
degraded in the lysosomes by acid hydrolases. A deficiency of any one of these
enzymes produces a sphingolipidosis, in which a characteristic sphingolipid
accumulates.
Prostaglandins (PGs) ,
thromboxanes (TXs), and leukotrienes (LTs) are produced in very small amounts
in almost all tissues, act locally, and have an extremely short half-life. They
serve as mediators of the inflammatory response. Arachidonic acid is the
immediate precursor of the predominant class of PGs in humans (those with two
double bonds). It is derived by the elongation and desaturation of the
essential fatty acid linoleic acid and is stored in the membrane as a component
of a phospholipid, generally PI. Arachidonic acid is released from the phospholipid
by phospholipase A2 (inhibited by cortisol). Synthesis of the PGs and TXs
begins with the oxidative cyclization of free arachidonic acid to yield PGH2
by prostaglandin endoperoxide synthase (PGH synthase), an endoplasmic reticulum
membrane protein that has two catalytic activities: fatty acid cyclooxygenase
(COX) and peroxidase. There are two isozymes of PGH synthase: COX-1
(constitutive) and COX-2 (nonconstitutive). Aspirin irreversibly inhibits both.
Opposing effects of PGI2 and TXA2 limit clot formation. LTs are linear
molecules produced from arachidonic acid by the 5-lipoxygenase pathway. They
mediate allergic response and are not inhibited by aspirin or other NSAIDs.
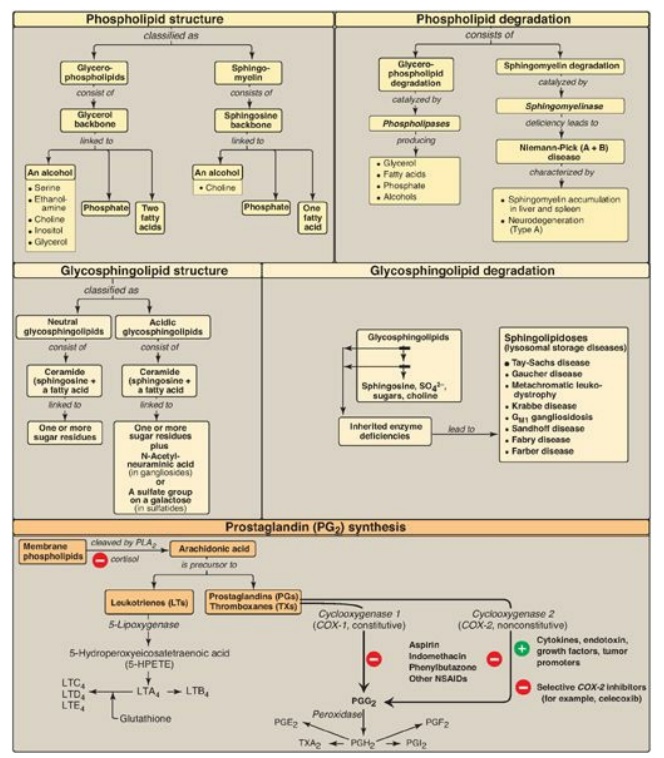
Figure 17.25 Key concept map
for complex lipids. PLA2 = phospholipase A2; SO42-
= sulfate ion; NSAIDs = nonsteroidal anti-inflammatory drugs.
Study Questions
Choose the ONE best answer.
17.1 Aspirin-induced asthma (AIA) is a severe
reaction to nonsteroidal anti-inflammatory drugs (NSAIDs) characterized by
bronchoconstriction 30 minutes to several hours after ingestion. Which of the
following statements best explains the symptoms seen in patients with AIA?
NSAIDs:
A. inhibit the activity
of the cystic fibrosis transmembrane conductance regulator protein, resulting
in thickened secretions that block airways.
B. inhibit cyclooxygenase but not lipoxygenase,
resulting in the flow of arachidonic acid to leukotriene synthesis.
C. activate the
cyclooxygenase activity of PGH synthase, resulting in increased synthesis of
prostaglandins that promote vasodilation.
D. activate
phospholipases, resulting in decreased amounts of
dipalmytoylphosphatidylcholine and alveolar collapse (atelectasis).
Correct answer = B. Nonsteroidal anti-inflammatory
drugs (NSAIDs) inhibit cyclooxygenase but not lipoxygenase, so any arachidonic
acid available is used for the synthesis of bronchoconstricting leukotrienes.
NSAIDs have no effect on the cystic fibrosis transmembrane conductance
regulator protein protein, defects in which are the cause of cystic fibrosis.
Steroids, not NSAIDs, inhibit phospholipase A2. Cyclooxygenase is inhibited by
NSAIDs, not activated. NSAIDs have no effect on phospholipases.
17.2 An infant, born at 28 weeks of gestation,
rapidly gave evidence of respiratory distress. Clinical laboratory and imaging
(X-ray) results supported the diagnosis of infant respiratory distress
syndrome. Which of the following statements about this syndrome is true?
A. It is unrelated to
the baby’s premature birth.
B. It is a consequence
of too few type II pneumocytes.
C. The lecithin/sphingomyelin
ratio in the amniotic fluid is likely to be greater than two.
D. The concentration of
dipalmitoylphosphatidylcholine in the amniotic fluid would be expected to be
lower than that of a full-term baby.
E. It is an easily
treated disorder with low mortality.
F. It is treated by
administering surfactant to the mother just before she gives birth.
Correct answer = D. Dipalmitoylphosphatidylcholine
(DPPC, or dipalmitoyl lecithin) is the lung surfactant found in mature, healthy
lungs. Respiratory distress syndrome (RDS) can occur in lungs that make too
little of this compound. If the lecithin/sphingomyelin ratio in amniotic is
greater than two, a newborn’s lungs are considered to be sufficiently mature
(premature lungs would be expected to have a ratio lower than two). The RDS
would not be due to too few type II pneumocytes, which would simply be
secreting sphingomyelin rather than DPPC at 28 weeks of gestation. The mother
is given a glucocorticoid, not surfactant, prior to giving birth. Surfactant
would be administered to the baby postnatally to reduce surface tension.
17.3 A 10-year-old boy was evaluated for burning
sensations in his feet and clusters of small, red-purple spots on his skin.
Laboratory studies revealed protein in his urine. Enzymic analysis revealed a
deficiency of α-galactosidase, and enzyme replacement therapy was recommended.
The most likely diagnosis is:
A. Fabry disease.
B. Farber disease.
C. Gaucher disease.
D. Krabbe disease.
E. Niemann-Pick
disease.
Correct answer = A. Fabry disease, a deficiency of
α-galactosidase, is the only X-linked sphingolipidosis. It is characterized by
pain in the extremities, a red-purple skin rash, and kidney and cardiac
complications. Protein in his urine indicates kidney damage. Enzyme replacement
therapy is available.
17.4 Current medical advice for individuals
experiencing chest pain is to call emergency medical services and chew a
regular-strength, noncoated aspirin. What is the basis for recommending
aspirin?
Aspirin has an
antithrombogenic effect: It prevents formation of blood clots that could
occlude heart vessels. Aspirin inhibits thromboxane A2 synthesis by
cyclooxygenase–1 in platelets through irreversible acetylation, thereby
inhibiting platelet activation and vasoconstriction. Chewing a noncoated
aspirin increases the rate of its absorption.
Related Topics
