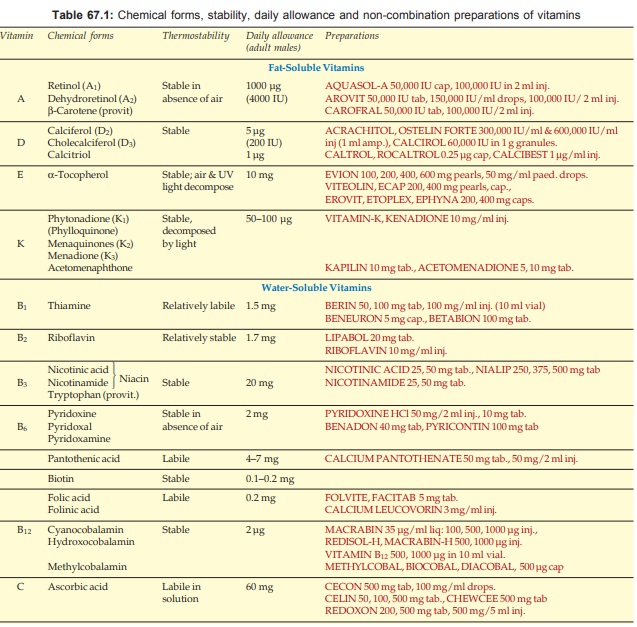
Watersoluble Vitamins
| Home | | Pharmacology |Chapter: Essential pharmacology : Vitamins
These are meagerly stored: excess is excreted with little chance of toxicity. They act as cofactors for specific enzymes of intermediary metabolism.
WATERSOLUBLE VITAMINS
THE VITAMIN B COMPLEX GROUP
Thiamine (Aneurine, vit B1)
Chemistry And Source
A colourless,
crystalline compound containing a
pyrimidine and a thiazole ring. It is present in the outer layers of cereals
(rice polishing), pulses, nuts, green vegetables, yeasts, egg and meat.
Absorption And Fate
Physiological amounts
are absorbed by active transport.
When large doses are given orally, some passive diffusion also occurs. Limited
amounts are stored in tissues. About 1 mg/day is degraded in the body, excess
is rapidly excreted in urine.
Physiological Role
After conversion in
the body to Thiamine pyrophosphate, it acts as a
coenzyme in carbohydrate metabolism: decarboxylation of ketoacids and hexose
monophosphate shunt. Requirement is dependent upon carbohydrate intake—about
0.3 mg/ 1000 K cal. It also appears to play some role in neuromuscular
transmission.
Pyrithiamine and oxythiamine are synthetic thiamine antagonists. Tea also contains
a thiamine antagonist.
Deficiency Symptoms
The syndrome of
thiamine deficiency beriberi is
seen in dry and wet forms:
Dry beriberi: Neurological
symptoms are prominent—polyneuritis with numbness, tingling, hyperesthesia,
muscular weakness and atrophy resulting in ‘wrist drop’, ‘foot drop’, paralysis
of whole limb, mental changes, sluggishness, poor memory, loss of appetite and
constipation.
Wet beriberi: Cardiovascular
system is primarily affected—palpitation,
breathlessness, high output cardiac failure and ECG changes. Protein deficiency
is commonly associated and adds to the generalised anasarka due to CHF.
Therapeutic Uses
Prophylactically (2–10 mg daily) in infants, pregnant women,
chronic diarrhoeas, patients on parenteral alimentation. Glucose infusion
unmasks marginal thiamine deficiency.
Beriberi—100 mg/day i.m. or i.v. till symptoms regress—then
maintenance doses orally.
Acute alcoholic intoxication: thiamine 100 mg is added to each
vac of glucose solution infused. Most neurological symptoms in chronic
alcoholics are due to thiamine deficiency—peripheral neuritis, Wernick’s
encephalopathy, Korsakoff’s psychosis: give 100 mg/day parenterally.
In neurological and cardiovascular disorders,
hyperemesis gravidarum, chronic anorexia and obstinate constipation—thiamine
has been used even without definite proof of its deficiency— symptoms improve
dramatically if thiamine deficiency has been causative.
Adverse Effects
Thiamine is nontoxic. Sensitivity reactions sometimes occur on
parenteral injection.
Riboflavin (vit B2)
Chemistry And Source
A yellow flavone compound found in milk, egg, liver, green leafy
vegetables, grains.
Absorption And Fate
Well absorbed by active transport and phosphorylated in
the intestine. Riboflavin phosphate (Flavin mononucleotide: FMN) is formed in
other tissues as well. Body does not significantly store riboflavin; larger doses
are excreted unchanged in urine. Thiamine and riboflavin are both synthesized
by colonic bacteria but this does not become available to the host.
Actions And Physiological Role
Flavin adenine dinucleotide (FAD) and flavin mononucleotide
(FMN) are coenzymes for flavoproteins involved in many oxidationreduction
reactions. Thiamine and riboflavin are devoid of pharmacological actions.
Deficiency Symptoms
Riboflavin deficiency generally occurs in association with other deficiencies.
Characteristic lesions are angular stomatitis; sore and raw tongue, lips,
throat, ulcers in mouth; vascularization of cornea. Dry scaly skin, loss of
hair; anaemia and neuropathy develop later.
Therapeutic Uses
To prevent and treat
ariboflavinosis (2–20 mg/day oral or parenteral), generally along with other B
complex members.
There is no proof of
benefit in any other condition.
Niacin (vit B3)
Chemistry And Source
Niacin refers to Nicotinic acid as well as Nicotinamide—pyridine compounds,
initially termed pellagra preventing factor. Sources are liver, fish, meat,
cereal husk, nuts and pulses.
The amino acid tryptophan
(mainly from animal protein) can be regarded as a provitamin, as it is
partially converted in the body to nicotinic acid (60 mg tryptophan = 1 mg
nicotinic acid). Maize eaters have suffered from pellagra because corn flour is
poor in tryptophan and it is believed to contain a niacin antagonist. Thus,
daily requirement of niacin is affected by the amount of tryptophan in diet.
Absorption And Fate
Niacin is completely
absorbed from gastrointestinal
tract. Physiological amounts are metabolized in the body, while large doses are
excreted unchanged in urine. Modest amounts are stored in liver.
Physiological Role And Actions
Nicotinic acid is readily converted to its amide which is a
component of the coenzyme Nicotinamide-adeninedinucleotide
(NAD) and its phosphate (NADP) involved in oxidation-reduction
reactions. These pyridine nucleotides act as hydrogen acceptors in the electron
transport chain in tissue respiration, glycolysis and fat synthesis.
Flavoproteins regenerate them by oxidizing NADH and NADPH.
Nicotinic acid (but not nicotinamide) in large doses is a vasodilator,
particularly of cutaneous vessels. It also lowers plasma lipids (see Ch. No. 45).
Deficiency Symptoms
Niacin deficiency produces ‘Pellagra’, cardinal manifestations
of which are:
Dermatitis—sunburn like dermal rash
on hands, legs and face which later
turn black, crack and peal.
Diarrhoea—with enteritis,
stomatitis, glossitis, salivation,
nausea and vomiting.
Dementia—with hallucinations preceded
by headache, insomnia, poor memory,
motor and sensory disturbances.
Anaemia and hypoproteinaemia are common in pellagra. Chronic
alcoholics are particularly at risk of developing pellagra, because in addition
to dietary deficiency, niacin absorption is impaired in them. Other B vitamin
deficiencies are often associated.
Therapeutic Uses
Prophylactically (20–50 mg/day oral) in people at risk of developing
pellagra.
Treatment of pellagra—200 to 500 mg/day in divided doses orally
or parenterally. Striking improvement occurs in 1–2 days, but skin lesions take
weeks to months. Nicotinamide is preferred, especially for injection, because
it does not cause flushing and other side effects seen with nicotinic acid.
Hartnup’s disease: in which tryptophan transport is impaired,
and in carcinoid tumours which use up tryptophan for manufacturing 5HT, need niacin
supplementation.
Nicotinic acid (not nicotinamide) has been used in peripheral
vascular disease and as hypolipidaemic (Ch. No. 45).
Adverse Effects
Nicotinic acid, in pharmacological doses, has many side effects
and toxicities. Nicotinamide is innocuous.
Pyridoxine (vit B6)
Chemistry And Source
Pyridoxine, Pyriodoxal and Pyridoxamine
are related naturally occurring pyridine compounds that have vit B6 activity.
Dietary sources are—liver, meat, egg, soybean, vegetables and whole grain.
Absorption And Fate
All three forms of the vitamin are well absorbed from the
intestine. They are oxidized in the body and excreted as pyridoxic acid. Little
is stored.
Physiological Role And Actions
Pyridoxine and pyridoxamine are readily oxidized to pyridoxal,
which is then phosphorylated to pyridoxal
phosphate—the coenzyme form. Pyridoxal dependent enzymes include
transaminases and decarboxylases involved in synthesis of nonessential amino
acids, tryptophan and sulfur containing amino acid metabolism, formation of 5HT,
dopamine, histamine, GABA and aminolevulinic acid (first step in the synthesis
of haeme). High protein diet increases pyridoxine requirement.
Pyridoxine has been shown to interact with steroid hormone receptors,
but its clinical implication is not clear. Prolonged intake of large doses of
pyridoxine can give rise to dependence, and mega doses (0.2–2.0 g/day) have
been linked with sensory neuropathy. Otherwise, pyridoxine is free from pharmacological
actions and side effects. However, suppression of lactation has been noted in nonsuckling
postpartal women given high doses of pyridoxine: may be due to increased
dopamine action on pituitary lactotropes.
Drug Interactions
Isoniazid reacts with pyridoxal to form a hydrazone, and thus inhibits
generation of pyridoxal phosphate. Isoniazid also combines with pyridoxal
phosphate to interfere with its coenzyme function. Due to formation of hydrazones,
the renal excretion of pyridoxine compounds is increased. Thus, isoniazid therapy
produces a pyridoxine deficiency state.
Hydralazine, cycloserine and penicillamine also interfere with
pyridoxine utilization and action.
Oral contraceptives reduce pyridoxal
phosphate levels in
some women.
Pyridoxine, by promoting formation of dopamine from levodopa in
peripheral tissues, reduces its availability in the brain, abolishing the
therapeutic effect in parkinsonism, but not when a peripheral decarboxylase
inhibitor is combined with it. 4-deoxypyridoxine is a vit B6 antagonist.
Deficiency Symptoms
Deficiency of vit B6 usually occurs in association with that of
other B vitamins. Symptoms ascribed to pyridoxine deficiency are—seborrheic
dermatitis, glossitis, growth retardation, mental confusion, lowered seizure
threshold or convulsions (due to fall in brain GABA levels), peripheral
neuritis and anaemia.
Therapeutic Uses
Prophylactically (2–5
mg daily) in alcoholics, infants and patients with deficiency of other B
vitamins.
To prevent and treat (10–50
mg/day) isoniazid, hydralazine and cycloserine induced neurological disturbances.
Acute isoniazid poisoning has been successfully treated with massive doses (in
grams) of pyridoxine.
To treat mental
symptoms in women on oral contraceptives (50 mg daily).
Pyridoxine responsive
anaemia (due to defective haeme synthesis) and homocystinuria are rare genetic
disorders that are benefited by large doses of pyridoxine (50–200 mg/day).
Convulsions in infants
and children.
Pantothenic Acid
Pantothenic acid is an
organic acid, widely distributed in food sources, especially liver, mutton, egg
yolk and vegetables. It is quickly absorbed and excreted unchanged in urine
with little storage.
It is a component of
coenzyme-A which functions in carbohydrate, fat, steroid and porphyrin metabolism
by catalysing acetate transfer reactions. Clinical deficiency of pantothenic
acid is not known. Experimental deficiency in man causes insomnia, intermittent
diarrhoea, flatulence, vomiting, leg cramps and paresthesias. Calcium/ sodium
pantothenate is included in B complex and multivitamin preparations. Intravenous
calcium pantothenate has been tried in paralytic ileus.
Biotin
Biotin is a sulfur containing organic acid found in egg yolk,
liver, nuts and many other Ch. No.s of food. Some of the biotin synthesized by
intestinal bacteria is also absorbed. It is well absorbed from intestine and
excreted mainly unchanged in urine. Not much is stored in the body. Avidin, a heat labile protein in egg
white, binds and prevents the absorption of biotin. Some other biotin antagonists
are also known. Biotin is a coenzyme for several carboxylases involved in
carbohydrate and fat metabolism. Deficiency symptoms include seborrheic
dermatitis, alopecia, anorexia, glossitis and muscular pain. Spontaneous
deficiency of biotin has been noted only in subjects consuming only raw egg
white and in patients on total parenteral nutrition. Except for these unusual
instances and rare genetic abnormalities of biotin dependent enzymes, there are
no clearly defined therapeutic uses of biotin. It is present in some multivitamin
preparations.
VITAMIN C (ASCORBIC ACID)
Chemistry And Source
Ascorbic acid is a 6 carbon organic acid with structural similarity
to glucose. It is a potent reducing agent and l-form is biologically active. Citrus fruits (lemons, oranges) and
black currants are the richest sources; others are tomato, potato, green
chillies, cabbage and other vegetables. Human milk is richer in vit C (25–50
mg/L) than cow’s milk.
Absorption And Fate
It is nearly
completely absorbed from g.i.t. and widely
distributed extra and intracellularly. Plasma concentration and total body
store of vit C is related to daily intake. The usual 60 mg/day intake results
in about 0.8 mg/dl in plasma and 1.5 g in the body as a whole. Increasing
proportions are excreted in urine with higher intakes. Body is not able to
store more than 2.5 g. It is partly oxidized to active (dehydroascorbic acid)
and inactive (oxalic acid) metabolites.
Physiological Role And Actions
Vit C plays a role in many oxidative and other metabolic
reactions, e.g. hydroxylation of proline and lysine residues of proto-collagen—essential
for formation and stabilization of collagen triple helix; hydroxylation of carnitine,
conversion of folic acid to folinic acid, biosynthesis of adrenal steroids,
catecholamines, oxytocin and vasopressin and metabolism of cyclic nucleotides
and prostaglandins. It directly stimulates collagen synthesis and is very
important for maintenance of intercellular connective tissue. A number of illdefined
actions have been ascribed to ascorbic acid in mega doses, but none is proven.
Deficiency Symptoms
Severe vit C
deficiency Scurvy, once prevalent among
sailors is now seen only in
malnourished infants, children, elderly, alcoholics and drug addicts. Symptoms
stem primarily from connective tissue defect: increased capillary
fragility—swollen and bleeding gums, petechial and subperiosteal haemorrhages,
deformed teeth, brittle bones, impaired wound healing, anaemia and growth retardation.
Therapeutic Uses
Prevention of ascorbic
acid deficiency in individuals at risk (see
above) and in infants: 50–mg/ day. Vit C or orange juice can be routinely
included in infant diet.
Treatment of
scurvy—0.5–1.5 g/day.
Postoperatively (500 mg
daily): though vit C does not enhance normal healing, suboptimal healing can be
guarded against. It has also been found to accelerate healing of bedsores and
chronic leg ulcers. Requirement of ascorbic acid is increased in postinjury
periods.
Anaemia: Ascorbic acid
enhances iron absorption and is frequently combined with ferrous salts (maintains
them in reduced state). Anaemia of scurvy is corrected by ascorbic acid, but it
has no adjuvant value in other anaemias.
To acidify urine (1 g
TDS–QID) in urinary tract infections (see
Ch. No. 54).
Large doses (2–6 g/day)
of ascorbic acid have been tried for a variety of purposes (common cold to
cancer) with inconsistent results. No definite beneficial effect has been noted
in asthma, cataract, cancer, atherosclerosis, psychological symptoms,
infertility, etc. However, severity of common cold symptoms may be somewhat
reduced, but not the duration of illness or its incidence. Improved working
capacity at submaximal workloads has been found in athletes but endurance is
not increased.
Adverse Effects
Ascorbic acid is well
tolerated in usual doses. Mega
doses given for long periods can cause ‘rebound scurvy’ on stoppage— probably
due to enhancement of its own metabolism or tissue acclimatization. The risk of
urinary oxalate stones may be increased. High doses may also be cytotoxic when
added to iron preparations.
