Liver
| Home | | Anatomy and Physiology | | Anatomy and Physiology Health Education (APHE) |Chapter: Anatomy and Physiology for Health Professionals: Digestive System
The liver is located in the upper right quadrant of the abdominal cavity, inferior to the diaphragm.
Liver
The liver is
located in the upper right quadrant of the abdominal cavity, inferior to the
diaphragm. It is the largest gland in the body, is reddish-brown, and is well
supplied with blood vessels. It extends from the level of the fifth intercostal
space to the lower margin of the ribs. The liver is enclosed in a fibrous
capsule and divided into lobes by connective tissue. The liver weighs about 1.4
kg or 3 pounds in an average adult. This wedge-shaped organ occu-pies most of
the right hypochondriac and epigastric abdominal regions. It is well protected
by the ribs, which nearly completely encase it.
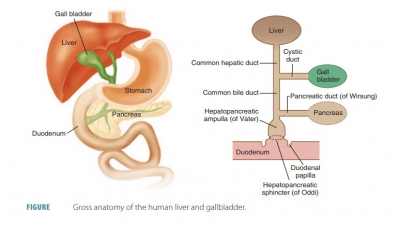
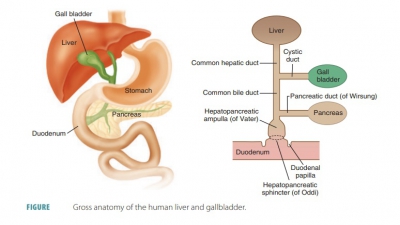
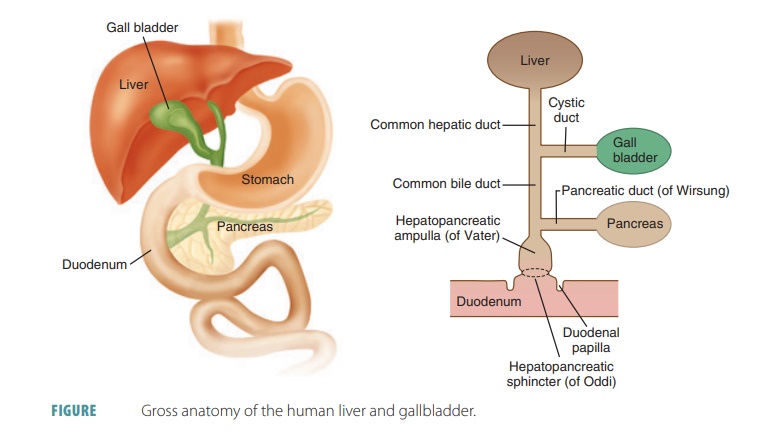
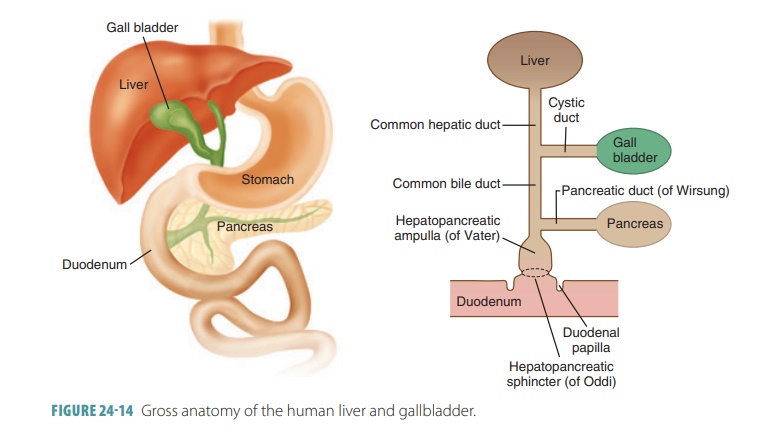
The right lobe of the liver is larger than its left lobe (FIGURE 24 -13). A deep fissure separates the right and left lobes. There are also two other lobes known as the caudate lobe and quadrate lobe, which are only visible when the liver is viewed inferiorly. The falciform ligament is a mesentery separating the right and left lobes anteriorly. It suspends the liver from the anterior abdominal wall and diaphragm. Around the inferior edge of the falciform ligament is the round ligament or ligamentum teres, which is a fibrous remnant formed from the fetal umbilical vein. The entire liver is enclosed by the visceral peritoneum, except for its bare, most superior area, which touches the diaphragm. At a point called the porta hepatis, the hepatic artery and hepatic portal vein enter the liver. The common hepatic duct also enters here and runs inferiorly from the liver (FIGURE 24-14). All these vessels travel through the lesser omentum.
Microscopic Structures of the Liver
Liver cells or hepatocytes adjust
circulating levels of nutrients through selective absorption and secretion.
Blood from the liver returns to the systemic circuit through the hepatic veins,
which open into the infe-rior vena cava. Hepatocytes are arranged within the
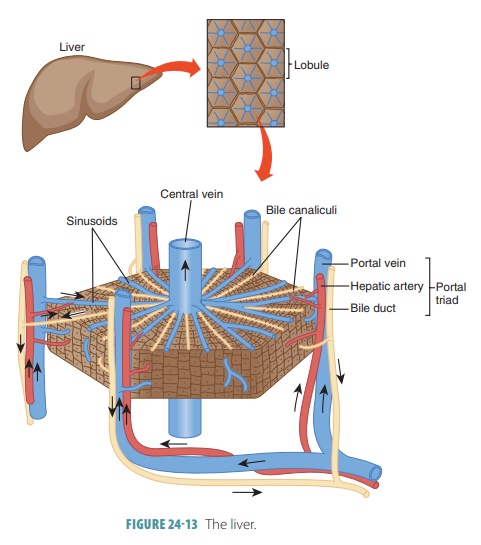
liver lobules into a series of plates radiating outward from the central vein.
Many tiny hepatic lobules make up
each lobe, and these lobules are the func-tional cells of the liver.
These lobules are about the size of sesame seeds, with six
sides. At each of the six corners, there is a portal triad or portal
tract region that
contains three primary
structures: a bile duct, a branch of the hepatic artery, and a branch of the
hepatic portal vein. Each lob-ule consists of many hepatic cells that radiate
out from a central vein. Plate-like groups of hepatic cells are sep-arated by
vascular channels called hepatic
sinusoids.
The hepatic portal vein carries blood from the digestive
tract, bringing newly absorbed nutrients into the sinusoids to nourish the
hepatic cells. Kupffer cells are large phagocytic macrophages attached to the inner hepatic sinusoids. They remove foreign
par-ticles such as bacteria that enter blood via the portal vein. Blood passes
from the sinusoids into the central veins of the hepatic lobules to leave the
liver.
Physiology of the Liver
The liver conducts many important activities of metabolism
and is responsible for three major types of functions: metabolic regulation,
hematologic regulation, and bile production. The liver actually has over 200
functions, but this discussion provides only a general overview. Hepatic cells
respond to hormones such as glucagon and insulin. Insulin converts glucose to
glycogen. Glucagon raises blood glucose levels by breaking down glycogen to
glucose or by converting noncarbohydrates into glucose.
The liver oxidizes fatty acids; synthesizes lipo-proteins,
phospholipids, and cholesterol; and con-verts parts of carbohydrate and protein
molecules into fat molecules. Fat from the liver is transported via the blood
to adipose tissue for storage. The liver is vital for protein metabolism as
well. It breaks down amino acids, forms urea, synthesizes plasma proteins such
as albumin, and converts some amino acids into others.
The liver stores glycogen, iron, and various vitamins,
including B12, A, and D. Liver macrophages or stellate macrophages destroy damaged erythrocytes and engulf foreign antigens. Toxic
substances are removed from the blood during detoxification and bile is secreted, which is important to
digestion. Secretions from the liver are carried to bile ductules by fine bile
canaliculi. The hepatic
ducts are formed from duct-ules of nearby lobules, which unite,
creating larger bile ducts. These ducts merge to form the common hepatic duct. The
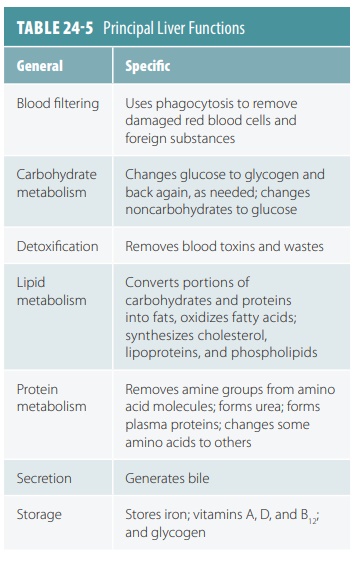
major functions of the liver are summarized
in TABLE 24-5.
The liver is amazing in its ability to regenerate. After surgical removal or other loss of up to 80% of its original mass, the liver can regenerate to its for-mer size within six to 12 months. Injury to the liver causes hepatocytes to secrete growth factors. These cause proliferations of endothelial cells that line the sinusoids and the release of other growth fac-tors. These additional growth factors influence the hepatocytes to multiply, so dead or dying liver tissue can be replaced.
Bile
Bile is
a fat emulsifier that is continuously secreted from hepatic cells. This yellow-green liquid
contains water, bile salts, the bile pigments bilirubin and biliverdin,
cholesterol, and electrolytes. It is alkaline in its pH. Bile salts make up most of these
elements and have a unique digestive function. Bile pigments develop from the
breakdown of hemoglobin in red blood cells and are normally excreted in the
bile. Up to 900 mL of bile can be secreted or generated by the hepatocytes
every day.
Only the bile salts and phospholipids play any role in the
digestive process. Bile salts are
derivatives of cholesterol that physically separate large fat globules that
enter the small intestine into millions of smaller fatty droplets in a process
known as emulsification. These
more accessible droplets create large surface areas for fat-digesting enzymes
to work with. The tiny fat droplets then mix with water and lipases digest them
more effectively as a result. Bile salts enhance absorption of cholesterol,
fatty acids, and fat-soluble vitamins A, D, E, and K. They also help to
solubilize cholesterol.
Bilirubin
Bilirubin is a waste product of the heme of hemo-globin
formed during breakdown of erythrocytes that have become older and worn out. It
is the pri-mary bile pigment. Although bilirubin is absorbed from the blood by
hepatocytes, excreted into the bile, and metabolized by resident bacteria in the
small intestine, the iron and globin from hemoglo-bin are saved and reused. In
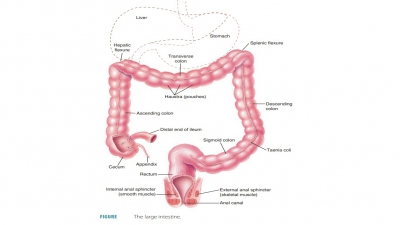
the large intestine, bil-irubin is converted by bacteria to urobilinogens and stercobilinogens. Some urobilinogens are absorbed
into the bloodstream for excretion via the urine. The remaining urobilinogens
in the colon are converted to urobilins,
and the remaining ster-cobilinogens are converted to stercobilins. Both of these conversions occur
from exposure to oxy-gen. In varying proportions, these pigments give the feces
its yellowish -brown or brown color. The meta-bolic activities of bacteria in
the colon create small amounts of intestinal gas, which is known as flatus.