Knee Joints
| Home | | Anatomy and Physiology | | Anatomy and Physiology Health Education (APHE) |Chapter: Anatomy and Physiology for Health Professionals: Support and Movement: Articulations
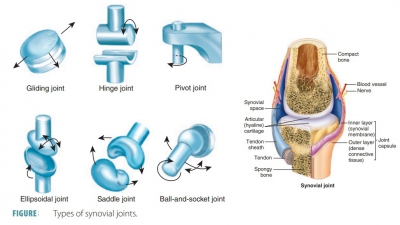
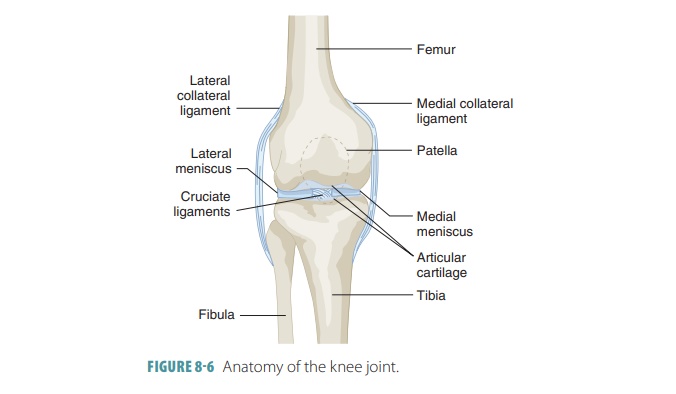
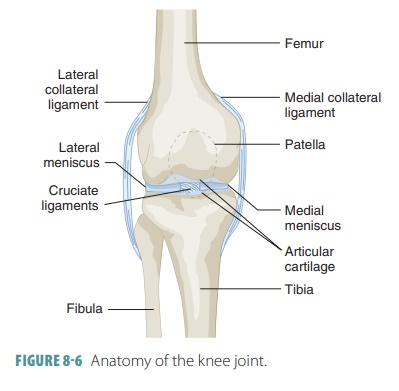
The knee joint has a single joint cavity, yet is the most complex joint in the body.
Knee Joints
The knee joint has a single joint
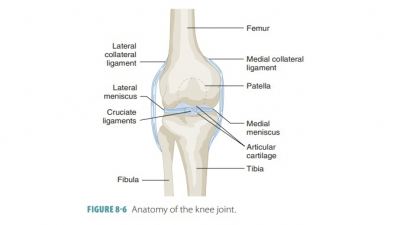
cavity, yet is the most complex joint in the body ( FIGURE
8-6). It is actually made up of an
intermediate joint between the patella and lower femur and lateral and medial
joints, collec-tively known as the tibiofemoral
joints. These joints lie between the
femoral condyles above and the semi-lunar
cartilages (C-shaped menisci) of the tibia below. The semilunar cartilages deepen the tibial articular sur-faces,
which are otherwise shallow. They absorb shock to the knee joint and also
prevent horizontal rocking of the femur on the tibia. Unfortunately, the
semilunar cartilages are often completely torn because they are only attached
at their outer margins. The menisci are damaged most commonly in athletic knee
injuries.
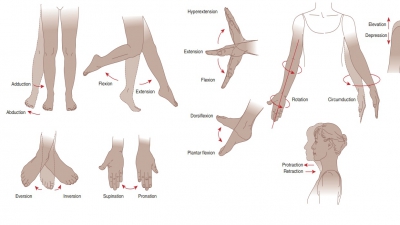
Flexion and extension is allowed
by the hinge-like tibiofemoral joint. In actuality, it is a bicondylar joint, with some rotation
occurring when the knee is slightly flexed or when it is extending. A fully
extended knee cannot rock horizontally or rotate without difficulty because of
strong ligament and menisci resistance. The patella glides across the femur’s
distal end during knee flexion because the femoropatellar joint is a plane joint.
The knee joint is the only articulation that has a cavity partially enclosed by a capsule. This capsule is thin and present only on the posterior aspects and sides of the knee. It covers most of the femoral and tibial condyles. It is absent anteriorly, and here, there are three broad ligaments running from the patella to the tibia below: the patellar, medial, and lateral patel-lar retinacula . They merge with the articular capsule on each side. Two of them (the patellar ligament and the lateral patellar retinacula) are continuations of the tendon from the quadriceps muscle in the ante-rior thigh. The patellar ligament is used to test the knee-jerk reflex.
The knee joint’s synovial cavity
is also complex, with various bursae. The subcutaneous
prepatellar bursa is an example
of a bursa that is often injured by trauma
to the anterior knee. The knee joint capsule is strengthened and stabilized by
all three types of joint ligaments. Two of these types (capsular and
extracap-sular) help to prevent hyperextension of the knee. They are tightly stretched when the knee is extended. When
the knee is extended, the extracapsular fibu-lar
and tibial collateral ligaments are
crucial to pre-vent lateral or medial rotation. The tibial
collateral ligament
is wide and flat, running from the
femur’s medial epicondyle to the tibial shaft’s medial condyle. This
ligament is fused to the medial meniscus. The posterior aspect of the knee
joint is partially stabilized by the oblique
popliteal ligament, which is part of
the tendon of the semimembranosus muscle. It fuses with the joint capsule. The
joint capsule is reinforced posteriorly by the arcuate
popliteal ligament, which has a
superior arc, from the head of the fibula over the popliteus muscle.
In the notch between the femoral condyles, the intracapsular ligaments (cruciate ligaments) cross each other to form an “X.” They provide
restraint against anterior–posterior displacement of the articular sur-faces.
These ligaments also secure the articulating bones during standing. They are in
the joint capsule but outside the synovial cavity. Therefore, the intra-capsular
ligaments are nearly covered by synovial membrane and run superiorly to the
femur. They are named for their tibial attachment site.
The anterior
cruciate ligament is attached to the tibia’s
anterior intercondylar area and passes upward, laterally, and posteriorly to
attach to the femur. Its actual point of attachment is the medial side of the
femur’s lateral condyle. The anterior cruciate ligament prevents the tibia
from sliding for-ward on the femur, controlling hyperextension of the knee. It
is tight during knee extension and slightly relaxed during knee flexion. The posterior cruciate ligament has more strength and is attached to the tibia’s posterior
intercondylar area. This ligament passes superiorly, medially, and anteriorly,
attaching to the lateral side of the medial condyle of the femur. It prevents
forward sliding of the femur or backward displacement of the tibia.
Many muscle tendons reinforce the
knee capsule. Muscle strength and tone protect the knee from injury. This is
especially true of the tendon of the semimem-branous muscle (posteriorly) and
the tendons of the quadriceps muscles in the anterior thigh.
When standing, the knees “lock
in” to provide steady support. As a person rises from a sitting to a standing
position, the wheel-like femoral condyles roll across the tibial condyles as
the flexed leg begins to extend at the knee. The lateral femoral condyle stops
rolling before the medial condyle stops. Therefore, the femur rotates medially
on the tibia, followed by twisting and tightening of the collateral and
cruciate ligaments of the knee. The menisci become compressed. Tension present
in the ligaments makes the joint become rigid. It cannot be flexed once more
until it is “unlocked,” which is accomplished by the popliteus muscle. This
muscle causes the ligaments to become slack and untwisted by rotating the femur
laterally on the tibia.