Higher Brain Functions
| Home | | Anatomy and Physiology | | Anatomy and Physiology Health Education (APHE) |Chapter: Anatomy and Physiology for Health Professionals: Central Nervous System
Although ongoing studies continue, the human brain’s higher functions are extremely difficult to truly understand.
Higher Brain
Functions
Although ongoing studies
continue, the human brain’s higher functions are extremely difficult to truly
understand. Brain waves are based on electrical activity, and normal brain functions involve
con-tinuous electrical activity of the neurons. Certain aspects of electrical
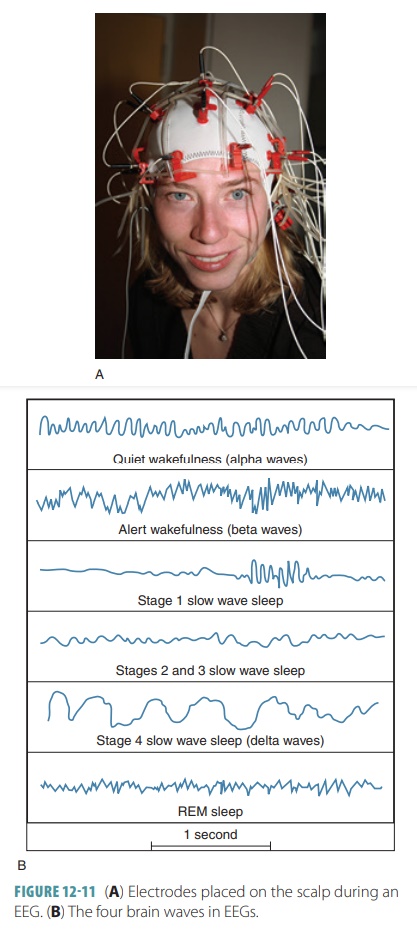
brain activity can be recorded on an electroencephalogram (EEG), which involves placing electrodes on the patient’s scalp. The EEG
measures voltage differences between the areas of the cerebral cortex. Brain
waves are the patterns of neuronal electrical activity that is recorded (FIGURES 12-11A and B). They are generated by the activity of synapses at the surface of the
cortex. Every individual’s brain wave patterns are unique but are grouped into
four primary types:
■■ Alpha waves: Relatively regular,
rhythmic, synchronous waves of low amplitude (8–13 Hz), they usually indicate
calm and relaxed wakefulness.
■■ Beta waves: Rhythmic but less
regular waves that have a higher frequency than alpha waves (14–30 Hz), they
occur during mental alertness such as when concentrating or looking at visual
stimuli.
■■ Theta waves: Irregular waves
that are more common in children and have a low frequency (4–7 Hz), they may
occur in adults when concentrating.
■■ Delta waves: High amplitude
(4 Hz or less) waves occurring in deep sleep or when something (such as
anesthesia) dampens the reticular activating system; if these waves exist in a
conscious adult, they indicate brain damage.
Brain waves change with brain
disease, aging, sensory stimuli, and the chemical balance of the body.
Consciousness
Consciousness
is defined as conscious perception of sensation,
capabilities related to higher mental pro-cessing, voluntary initiation, and
control of move-ment. Consciousness levels are graded based on alertness, drowsiness or lethargy, stupor, and coma. It involves
simultaneous activity of large portions of the cerebral cortex and is
superimposed on other types of neural activity (both motor control and
cognition). It is holistic and completely interconnected, for example, a memory
triggered by a location, an odor, a person, or other stimuli.
Sleep and Sleep Patterns
Sleep is a state of partial
unconsciousness from which we may be
aroused by stimulation. It is dif-ferent from coma, from which a person cannot be aroused by stimulation. During
sleep, most cortical activity is depressed, but brain stem functions con-tinue.
These functions include control of heart rate, blood pressure, and respiration.
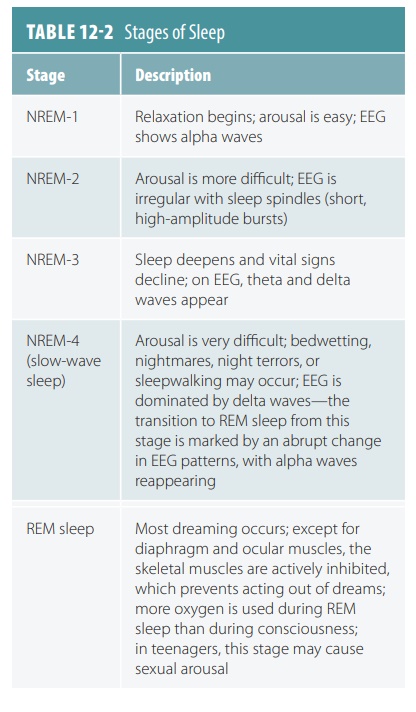
The two major types of sleep are non-rapid
eye movement (NREM) sleep and rapid eye movement (REM) sleep. Each of
these has different patterns on an EEG. TABLE
12-2 lists the stages of sleep.
Sleep patterns are normally based
on a natural 24-hour circadian rhythm.
The sleep cycle is con-trolled by the hypothalamus. Sleep occurs because of the
inhibition of the brain stem’s reticular activat-ing system. The preoptic
nucleus is the actual com-ponent that turns off arousal and puts the cerebral
cortex to sleep.
Sleep patterns alternate through
most of the sleep cycle. There are four stages of NREM sleep and also REM
sleep. As NREM and REM sleep alternate, partial arousals occur
occasionally. These are defined by their EEG patterns. In the first 30–45
minutes of sleep, the first two stages of NREM pass, followed by stages 3 and
4, which are known as slow -wave sleep. This type of sleep is thought to have restor-ative
properties for the mind and body. As a result, sleep
-deprived people will spend more time in slow-wave sleep the next time they do
fall asleep. After these stages, as the sleep patterns deepen, the fre-quency
of EEG waves declines while their amplitude increases. There are progressive
decreases in blood pressure and heart rate.
After about 90 minutes, once NREM
stage 4 has been reached, there is an abrupt change in EEG patterns, which
become irregular. There is a quick backtracking
through the sleep stages until alpha waves
reappear. The alpha waves are more typical of brain activity when we are awake.
This return of alpha waves indicates the onset of REM sleep. There are
increases in heart and respiratory rates, along with blood pressure. There is
a decrease in motility inside the gastrointestinal tract. During REM sleep, the
brain uses more oxygen than during waking hours. The skeletal muscles are limp
due to active inhibition, but the eyes move quickly underneath the eyelids. The
majority of dreaming occurs during REM sleep. The body’s temporary paralysis
keeps us from acting out what we are dreaming.
Sleep Regulation
Sleep and wakefulness cycles
occur in a natural 24-hour or circadian
rhythm. The hypothalamus regulates the timing of sleep cycles. Its suprachias-matic nucleus acts like the
body’s clock to regulate the
sleep-inducing area called the preoptic
nucleus. As the reticular activating system inside the brain stem is
inhibited, the preoptic nucleus causes the cerebral cortex to enter sleep. The
arousal system is switched off, and the RAS centers help maintain the awake
state as well as dreaming and other sleep stages. Just prior to awakening,
hypothalamic neu-rons release orexins,
which are peptides that function as “waking up” chemicals. Therefore, some
brain stem reticular formation neurons fire at heightened rates, arousing the
cerebral cortex. Many chemicals in the body are linked to sleepiness; the
importance of their functions is not fully understood.
Sleep Deprivation
Deprivation of REM sleep causes
depression and moodiness, resulting in various personality dis-orders. Dreaming
may help an individual to focus thoughts while awake. REM sleep helps the brain
analyze life events and manage emotional problems via dream images. It also
eliminates synaptic con-nections that are not needed. Dreaming actually helps
us to forget problematic occurrences. The need for sleep declines from infancy
(from approx-imately 16 hours per day) to reach a plateau of 7.5–8.5 hours (in
early adulthood), and then declines again in old age. Sleep patterns may
change differently throughout life for every individual. Stage 4 sleep
declines steadily over time and may not even occur in elderly individuals. REM
sleep occupies about 50% of the sleep of infants but declines to about 25% in
adults.
1.
What are the four primary types of brain wave patterns?
2.
What are the two major types of sleep?
3.
What are the results of REM sleep deprivation?
4.
What are the functions of Broca’s area and Wernicke’s area?
Language Functions
In the brain, language involves
nearly all the left asso-ciation cortex, especially Broca’s area and Wernicke’s area. Lesions of Broca’s
area may cause difficulty speak-ing, writing, typing, or using sign language.
Lesions of Wernicke’s area may cause lack of understanding of language or the
use of excessive nonsense words while speaking. Language, as controlled by the
brain, also involves the basal nuclei and surrounding portions of the cerebral
cortex. The right association cortex is involved in nonverbal language or body
language.
Memory Functions
Memory involves storage and retrieval of informa-tion and is
required for learning, establishing behav-iors, and normal conscious activity.
Short -term memory (working memory) focuses on small pieces of information needed
for a few moments and is based on approximately seven to eight groups of
information. Long -term
memory may be unlim-ited,
but is affected by changes to the body over time and declines with aging. The
transfer of information from short-term to long-term memory is influenced by
your emotional state, rehearsing or repeating material, associating new
information to stored infor-mation, and automatic memory (which is the
uncon-scious memorizing of something that occurred such as what a person was
wearing).
Memories that are transferred to
long-term memory become permanent over time. Memory consolidation appears to involve “inserting” new facts into areas of
knowledge previously stored in the cerebral cortex. This process is primarily
han-dled by the hippocampus and surrounding temporal cortical areas. They
communicate with the prefrontal cortex and thalamus during these functions.
How-ever, widespread amnesia occurs if there is bilateral destruction.
Consolidated memories are retained, yet new sensory input is not associated
with older sensory input. The individual lives in the present time with little
ability to connect with the past, a con-dition known as anterograde amnesia. If a physi-cian consulted a patient with anterograde amnesia,
then left the room and returned a short while later, the patient would not
remember the physician. The loss of memories from the distant past is called retrograde amnesia.
It is believed that certain portions
of every memory are stored close to areas of the brain that need to utilize
them. In this manner, new sensory input can be quickly related to older sensory
input of a similar type. For example, musical memory is stored in the temporal
cortex, while visual memories are stored in the occipital cortex.