Ethyl Alcohol
| Home | | Pharmacology |Chapter: Essential pharmacology : Ethyl and Methyl Alcohols
Alcohols are hydroxy derivatives of aliphatic hydrocarbons. When unqualified, ‘alcohol’ refers to ethyl alcohol or ethanol. Pharmacology of alcohol is important for its presence in beverages (which have been used since recorded history) and for alcohol intoxication, rather than as a drug.
ETHYL ALCOHOL
(Ethanol)
Alcohols are hydroxy
derivatives of aliphatic hydrocarbons. When unqualified, ‘alcohol’ refers to ethyl alcohol or ethanol. Pharmacology of alcohol is important for its presence in
beverages (which have been used since recorded history) and for alcohol intoxication,
rather than as a drug.
Alcohol is
manufactured by fermentation of sugars:

Fermentation proceeds
till alcohol content reaches ~ 15%. Then the reaction is inhibited by alcohol
itself. Starchy cereals, e.g. barley, when soaked produce malt:

which can then be
fermented by yeast to produce alcohol. The major source of commercial alcohol
is mollases, a byproduct of sugar
industry.
Alcoholic Beverages
There are a large
variety of alcoholic beverages.
A. Malted Liquors
Obtained by fermentation
of germinating cereals; are undistilled—alcohol content is low (3–6%) e.g.
Beers, Stout. Now strong beers (upto 10%) are also available.
B. Wines
Produced by fermentation of natural sugars as present in grapes and other fruits. These
are also undistilled.
Light wines Claret, Cider; alcohol content 9–12%, cannot exceed 15%.
Fortified wines Port, Sherry (alcohol 16–22%): distilled beverages are added from outside.
Effervescent wines Champagne (12–16% alcohol): bottled before fermentation is complete.
Wines are called ‘dry’ when all sugar present has been fermented
and ‘sweet’ when some is left.
C. Spirits
These are distilled after fermentation; e.g. Rum, Gin, Whiskey, Brandy, Vodka etc. Though
the alcohol content of these can vary from 40–55%, in India (and almost internationally)
for all licenced brands it is standardized to 42.8% v/v or 37% w/w.
The taste, flavour and value of alcoholic beverages depends not
only on alcohol content but on the presence of higher ethers, higher alcohols,
aldehydes, esters, polymers, and volatile oils; many of these are formed during
‘maturation’ of the beverage.
Other Forms Of
Alcohol
1. Absolute alcohol 99% w/w ethanol
(dehydrated alcohol).
2. Rectified spirit 90% w/w ethyl alcohol—from mollases, by
distillation.
3. Proof spirit It is an old term. If whisky is poured on gun powder and
ignited and it explodes, then it was labelled to be of ‘proof strength’. If
water is mixed to it, gun powder will not ignite. 100% proof spirit is 49.29%
w/w or 57.1% v/v alcohol
Pharmacological Actions
1. Local Actions
Ethanol is a mild
rubefacient and counterirritant
when rubbed on the skin. By evaporation it produces cooling. Applied to
delicate skin (scrotum) or mucous membranes it produces irritation and burning
sensation; should not be applied in the mouth, nose, etc. Injected s.c. it
causes intense pain, inflammation and necrosis followed by fibrosis. Injected
round a nerve it produces permanent damage.
Alcohol is an astringent—precipitates surface proteins and
hardens skin. By precipitating bacterial proteins it acts as an antiseptic. The
antiseptic action increases with concentration from 20 to 70%, remains constant
from 70 to 90% and decreases above that. That 100% ethanol is more dehydrating
but poorer antiseptic than 90% ethanol, shows that antibacterial action is not
due to dehydration of bacterial protoplasm. Alcohol does not kill bacterial
spores.
2. CNS
Alcohol is a neuronal
depressant. Since the highest
areas are most easily deranged and these are primarily inhibitory—apparent
excitation and euphoria are experienced at lower plasma concentrations (30–100
mg/dl). Hesitation, caution, self-criticism and restraint are lost first. Mood
and feelings are altered; anxiety may be allayed. With increasing concentration
(100–150mg/dl) mental clouding, disorganization of thought,
impairment of memory and other faculties, alteration of perception and
drowsiness supervene. At 150–200 mg/dl the person is sloppy, ataxic and drunk;
200–300 mg/dl result in stupor and above this unconsciousness prevails, medullary
centres are paralysed and death may occur. Though, alcohol can produce
anaesthesia, margin of safety is narrow.
Any measurable concentration of alcohol produces a measurable
slowing of reflexes: driving is dangerous. Performance is impaired, fine
discrimination and precise movements are obliterated; errors increase, except
if fear of punishment and anxiety of failure has already impaired
it—performance may be improved by allaying of anxiety and fear.
Effects of alcohol are more marked when the concentration is rising
than when it is falling. Some consider it to be a reflection of acute
tolerance.
Alcohol can induce sleep but is not a dependable hypnotic. Some
individuals report poor quality of sleep and early morning awakening. Sleep
architecture may be disorganized and sleep apnoea aggravated. Alcohol raises
pain threshold and also alters reaction to it, but is not a dependable
analgesic—severe pain can precipitate confusion and convulsions. During the
time alcohol is acting on brain, it exerts anticonvulsant action, but this is
followed by lowering of threshold: seizures may be precipitated in epileptics.
Chronic alcohol abuse damages brain neurones.
The cortex and the reticular activating system are most
sensitive to alcohol; other areas get depressed as concentration rises.
Mechanism Of Action
Alcohol was believed
to produce CNS depression by a
generalized membrane action altering the state of membrane lipids. However,
recently specific effect on multiple receptor operated ion channels has been
demonstrated at concentrations attained during moderate drinking. Alcohol
promotes GABAA receptor mediated synaptic inhibition (through
chloride channel opening) as well as inhibits NMDA and kainate type of
excitatory amino acid receptors (operating through cation channels). Action of
5HT on 5HT3 inhibitory auto-receptor (having an intrinsic ion
channel) is augmented. Some studies suggest that cerebral nicotinic cholinergic
receptors (operating through Na+ channel) may also be the targets of alcohol action.
Ethanol can indirectly reduce neurotransmitter release by inhibiting voltage
sensitive neuronal Ca2+ channels. Blockade of adenosine uptake by alcohol could
also contribute to synaptic depression. Turnover of NA in brain is enhanced by
alcohol through an opioid receptor dependent mechanism. This is probably
important in the pleasurable effects of alcohol and in the genesis of alcohol
dependence. Activity of membrane bound enzymes like Na+ K+ ATPase and adenylyl
cyclase is also altered. The activity and translocation of channel/enzyme
proteins in the membrane could be affected by alcohol through protein kinase C
(PKC) and protein kinase A (PKA) mediated alteration in the state of their phosphorylation.

3. CVS
The effects are
dependent on dose.
Small doses: produce only cutaneous (especially on the face) and gastric
vasodilatation. Skin is warm and flushed and there may be conjunctival
injection; BP is not affected.
Moderate doses: cause tachycardia and a mild rise in BP due to increased muscular
activity and sympathetic stimulation.
Large doses: cause direct myocardial as well as vasomotor centre depression and there
is fall in BP.
Epidemiological studies have confirmed that chronic alcoholism
contributes to hypertension and can lead to cardiomyopathy. Atrial fibrillation
and other cardiac arrhythmias may occur due to conduction defects and QT prolongation.
4. Blood
Regular intake of small to moderate amounts of alcohol has
been found to raise HDLcholesterol levels and decrease LDL oxidation. This may
be responsible for the 15–35% lower incidence of coronary artery disease in
such individuals. Risk reduction is greatest in high risk subjects and
protection is lost if > 3 drinks are consumed daily. Megaloblastic
anaemia has been seen in chronic alcoholism due to interference with folate
metabolism.
5. Body Temperature
Alcohol is reputed to combat cold. It does
produce a sense of warmth due to cutaneous and gastric vasodilatation, but heat
loss is actually increased in cold surroundings. High doses depress temperature
regulating centre.
6. Respiration
Brandy or whiskey are reputed as respiratory
stimulants in collapse. They irritate buccal and pharyngeal mucosa—may transiently
stimulate respiration reflexly. However, it is better not to depend on this,
because the direct action of alcohol on respiratory centre is only a depressant
one.
7. GIT
Alcoholic beverages have variable effect on gastric secretion depending on the beverage
itself and whether the individual likes it. However, dilute alcohol (optimum
10%) put in the stomach by Ryle’s tube is a strong stimulant of gastric
secretion (especially of acid). It acts directly as well as reflexly. Higher
concentrations (above 20%) inhibit gastric secretion, cause vomiting, mucosal
congestion and gastritis. Alcoholism is an important cause of chronic
gastritis. Lower esophageal sphincter (LES) tone is reduced by alcohol—may
accentuate reflux. Bowel movements may be altered in either direction. Acute pancreatitis
is a complication of heavy drinking.
8. Liver
Neither alcohol intoxication nor chronic use of moderate amounts cause significant
liver damage, provided adequate nutrition is maintained. However, it does
mobilize peripheral fat and increases fat synthesis in liver in a dose-dependent
manner. Proteins may also accumulate in liver because their secretion is
decreased. Chronic alcoholism subjects liver to oxidative stress and causes
cellular necrosis followed by fibrosis. Acetaldehyde produced during metabolism
of alcohol appears to damage the hepatocytes and induce inflammation, especially
on chronic ingestion of large amounts. Increased lipid peroxidation and
glutathione depletion occurs. These combined with vitamin and other nutritional
deficiencies may be responsible for the so called alcoholic cirrhosis.
Regular alcohol intake induces microsomal enzymes.
9. Skeletal muscle
Alcohol produces little direct effect. Fatigue is allayed by small
doses, but muscle work is increased or decreased depending on the predominating
central effect. Weakness and myopathy occurs in chronic alcoholism.
10. Kidney
Diuresis is often
noticed after alcohol intake. This is
due to water ingested with drinks and alcohol induced inhibition of ADH
secretion. It does not impair renal function.
11. Sex
Alcohol is reputed as an aphrodisiac. Aggressive sexual
behaviour is due to loss of restraint and inhibition. However, performance of
the sexual act is often impaired. Chronic alcoholism can produce impotence,
testicular atrophy, gynaecomastia and infertility.
12. Endocrine Effects
Moderate amounts of alcohol increase Adr
release which can cause hyperglycaemia and other sympathetic effects. However,
acute intoxication is often associated with hypoglycaemia and depletion of
hepatic glycogen, because gluconeogenesis is inhibited. Glucagon, thus fails to
reverse it and glucose must be given.
13. Uterine contractions are suppressed at moderate blood
levels.
Pharmacokinetics
Rate of alcohol absorption from the stomach is dependent on its
concentration, presence of food, and other factors, but is generally quite
slow. Absorption from intestines is very fast; peak levels are attained after
~30 min. Thus, gastric emptying determines rate of absorption. Limited first
pass metabolism occurs in stomach and liver. Absorption of alcohol from skin of
adults is minimal but may be significant in infants given alcohol sponges.
Alcohol gets distributed widely in the body (vol of distribution
0.7 L/kg), crosses blood brain barrier efficiently: concentration in brain is
very near blood concentration. It also crosses placenta freely. It is oxidized
in liver to the extent of 98%. Even with high doses, not more than 10% escapes
metabolism.
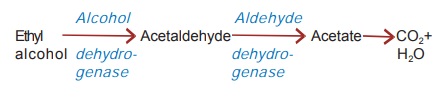
In addition to alcohol
dehydrogenase, small amounts of alcohol are oxidized by hepatic microsomal
enzymes as well. Metabolism of alcohol follows zero order kinetics, i.e. a constant amount (8–12 ml of absolute
alcohol/ hour) is degraded in unit time, irrespective of blood concentration.
Thus, rate of consuming drinks governs whether a person will get drunk.
Excretion of alcohol
occurs through kidney and lungs, but neither is quantitatively significant.
Concentration in exhaled air is about 0.05% of blood concentration: this is
utilized for medicolegal determination of drunken state. The subject blows in a
balloon and alcohol is measured by portable breath analyser.
Interactions
1. Alcohol synergises
with anxiolytics, antidepressants, antihistaminics, hypnotics, opioids → marked CNS depression
with motor impairment can occur: Chances of accidents increase.
2. Individuals taking
sulfonylureas (especially chlorpropamide), certain cephalosporins
(cefoperazone, moxalactam, cefamandole) and metronidazole have experienced
bizarre, somewhat disulfiramlike reactions when they consume alcohol.
3. Acute alcohol
ingestion inhibits, while chronic intake induces tolbutamide, phenytoin (and
many other drugs) metabolism.
4. Insulin and sulfonylureas:
alcohol enhances hypoglycaemia acutely.
5. Aspirin and other
NSAIDs cause more gastric bleeding when taken with alcohol.
6. Alcoholics are more
prone to paracetamol toxicity due to enhanced generation of its toxic metabolite.
Food Value
Alcohol requires no digestion and is metabolized rapidly. It is
an energy yielding substrate: 7 Cal/g, but these cannot be stored. It also does
not supply body building and other essential constituents of food. Those who
consume substantial part of their caloric intake as alcohol, often suffer from
nutritional deficiencies. Thus, alcohol is an imperfect and expensive food.
Contraindications
Alcohol is seldom prescribed medically. However, its consumption
should be avoided by—
1. Peptic ulcer,
hyperacidity and gastroesophageal reflux patients (alcohol increases gastric
secretion and relaxes LES).
2. Epileptics: seizures
may be precipitated.
3. Severe liver disease
patients.
4. Unstable personalities:
they are likely to abuse it and become excessive drinkers.
5. Pregnant women: Even
moderate drinking during pregnancy can produce foetal alcohol syndrome resulting
in intrauterine and postnatal growth retardation, low IQ, microcephaly, facial
and other abnormalities, and immunological impairment→increased susceptibility
to infections. Heavy drinking by mother in addition increases the incidence of
miscarriage, stillbirths and low birthweight babies.
Guidelines For Safe Drinking
Physicians are often asked to advise
on safe ways of drinking. Various official agencies, physician organizations
and alcoholism experts have putforth guidelines in this regard, but they are
not uniform. The following may be concluded:
·
On an average 1–2 drinks per day is usually
safe.
·
Not more than 3 drinks on any one occasion.
·
Consumption of >3 drinks per day is associated
with documented adverse health effects.
·
Do not drive or engage in hazardous activities
after drinking.
·
Do not drink if an interacting drug has been
taken.
·
Subjects with any contraindication should not
drink.
·
Safe limits are somewhat lower for women than
for men, because metabolism of alcohol is slower and its bioavailability higher
(due to less first pass metabolism in stomach) in women than in men.
[Note: 1 drink = 50 ml
of spirits = 150 ml of wines = 400 ml of beer; all have roughly 18 g alcohol,
which taken in empty stomach produces a peak alcohol blood level of ~ 25 mg/dl
in an adult male of average built.]
Toxicity
A. Side Effects Of
Moderate Drinking Nausea, vomiting, flushing,
hangover, traffic accidents.
B. Acute Alcoholic
Intoxication Hypotension, gastritis, hypoglycaemia, collapse,
respiratory depression, coma and death.
Treatment: Gastric lavage is
helpful only when the patient is
brought soon after ingesting alcohol, which is rare. Since most patients are
disoriented or comatose, the first priority is to maintain patent airway and
prevent aspiration of vomitus. Tracheal intubation and positive pressure
respiration may be needed if it is markedly depressed. Analeptics should not be
used—may precipitate convulsions. Most patients will recover with supportive
treatment, maintenance of fluid and electrolyte balance and correction of
hypoglycaemia by glucose infusion till alcohol is metabolized. Thiamine (100 mg
in 500 ml glucose solution infused i.v.) should be added. Recovery can be
hastened by haemodialysis. Insulin + fructose drip has been found to accelerate
alcohol metabolism. However, its clinical impact is not remarkable.
C. Chronic
Alcoholism On chronic intake, tolerance develops to subjective and
behavioral effects of alcohol, but is generally of a low degree. It is both
pharmacokinetic (reduced rate of absorption due to gastritis and faster
metabolism due to enzyme induction) and cellular tolerance. Psychic dependence
often occurs even with moderate drinking; depends a lot on individual’s likings
and attitudes.
Recent studies have confirmed that a genetic basis contributes
to progression from social drinking to alcoholism in about 50% individuals.
Alcoholism is often a familial trait. Some differences in sensitivity of
various neuronal systems to alcohol among ‘predisposed’ and ‘not predisposed’
individuals have been demonstrated.
There is no single
explanation for why people drink. Diverse feelings and behaviours are provoked
by alcohol in different individuals and in the same individual on different
occasions. Alcohol can make people happy as well as sad, curtious as well as
mean, talkative as well as silent, friendly as well as hostile. All this cannot
be explained on the basis of pharmacological actions of alcohol alone.
Attitudes, beliefs, peer groups, social setting and learned experiences all
have a bearing. Alcohol is said to produce good mood, sense of wellbeing, self
confidence, sociability, etc. But these infact are learned behaviours. In some
societies, alcoholic beverages have become an acceptable form of extending
courtesy and of entertainment. Drinking is often related to ‘celebration’ and
‘high living’. There is ‘wine snobbery’ in high social groups.
To some, excess drinking provides the excitement of risk taking.
People often boast of their capacity to drink. To the young, drinking may be a
symbol of rebellion against the oppressive older generation and rejection of
the values of the establishment. ‘Binge drinking’ is a specific behavioural
pattern of bouts of excessive drinking. Alcohol is often an excuse for bad
behaviour. Society’s view that intoxicated person is unaware of his actions—
makes intoxication an attractive state, because there is increased freedom of
what one can say or do after drinking. Thus, there are a variety of motivations
for drinking.
Physical dependence
occurs only on heavy and roundtheclock drinking (if alcohol is present in the
body continuously). Heavy drinking is often associated with nutritional
deficiencies, because food is neglected and malabsorption may occur. In
addition to impaired mental and physical performance, neurological afflictions
are common—polyneuritis, pellagra, tremors, seizures, loss of brain mass,
Wernicke’s encephalopathy, Korsakoff’s psychosis and megaloblastic anaemia.
Alcoholic cirrhosis of liver, hypertension, cardiomyopathy, CHF, arrhythmias,
stroke, acute pancreatitis, impotence, gynaecomastia, infertility and skeletal
myopathy are other complications. Incidence of oropharyngeal, esophageal and
hepatic malignancy and respiratory infections is high; immune function is
depressed.
Withdrawal Syndrome consists of anxiety,
sweating, tremor, impairment of sleep, confusion, hallucinations, delirium
tremens, convulsions and collapse.
Treatment Psychological and
medical supportive measures are needed during withdrawal. Many CNS depressants
like barbiturates, phenothiazines, chloral hydrate have been used as substitution
therapy in the past (to suppress withdrawal syndrome) but benzodiazepines
(chordiazepoxide, diazepam) are the preferred drugs now. These have a long
duration of action and can be gradually withdrawn later.
Naltrexone:
Several studies have demonstrated involvement of opioid system in the pleasurable reinforcing effects
of alcohol probably by blunting dopamine mediated reward function. Trials among
postaddicts have shown that the long acting opioid antagonist naltrexone helps prevent relapse of
alcoholism. It reduced alcohol craving, number of drinking days and chances of
resumed heavy drinking. Naltrexone is approved by USFDA for use as adjuvant in
comprehensive treatment programmes for alcohol dependent subjects and is being
used in India at most deaddiction centres, after the individual has undergone
withdrawal and is motivated.
Acamprostate It is a weak NMDAreceptor
antagonist with modest GABAA
receptor agonistic activity that is being used in Europe for maintenance
therapy of alcohol abstinence. In conjunction with social and motivational therapy,
it has been found to reduce relapse of the drinking behaviour. The efficacy of
acomprostate in this regard is rated comparable to naltrexone.
The 5HT3
antagonist ondansetron and the
antiepileptic topiramate have also
shown some promise in treating alcoholism.
Clinical Uses
Medicinal uses of
ethanol are primarily restricted to external application and as a vehicle for
liquid preparations used internally.
a)
As antiseptic (see Ch. No. 65).
b) Rubefacient and
counterirritant for sprains, joint pains, etc.
c) Rubbed into the skin
to prevent bedsores. It should not be applied on already formed sores.
Astringent action of alcohol is utilized in antiperspirant and aftershave
lotions.
c)
Alcoholic sponges to reduce body temperature
in fever. However, cold water/ice may be better.
d) Intractable neuralgias
(trigeminal and others), severe cancer pain—injection of alcohol round the
nerve causes permanent loss of transmission.
e)
To ward off cold—may benefit by causing
vasodilatation of blanched mucosae; but further exposure after taking alcohol may
be deleterious because alcohol increases heat loss due to cutaneous
vasodilatation.
f)
As appetite stimulant and carminative: 30– 50
ml of 7–10% alcohol may be taken as beverages or tinctures before meal.
g) Reflex stimulation in
fainting/hysteria: 1 drop in nose.
h) To treat methanol
poisoning.
Aldehyde Dehydrogenase Inhibitors
Disulfiram
It inhibits the enzyme
aldehyde dehydrogenase probably
after conversion into active metabolites. When alcohol is ingested after taking
disulfiram, the concentration of acetaldehyde in tissues and blood rises and a
number of highly distressing symptoms (aldehyde syndrome) are produced
promptly. These are— flushing, burning sensation, throbbing headache,
perspiration, uneasiness, tightness in chest, dizziness, vomiting, visual
disturbances, mental confusion, postural fainting and circulatory collapse.
Duration of the syndrome (1–4 hours) depends on the amount of alcohol consumed.
Because of risk of severe reaction, disulfiram is infrequently used.
Disulfiram has been used as an aversion technique in chronic
alcoholics who are motivated and sincerely desire to leave the habit. After
abstaining from alcohol overnight, disulfiram is given 1 g on 1st day, 0.75 g
on 2nd day, 0.5 g on 3rd and 0.25 g subsequently. Sensitization to alcohol
develops after 2–3 hours of first dose, reaches its peak at ~12 hours and lasts
for 7–14 days after stopping it, because inhibition of aldehyde dehydrogenase
with disulfiram is irreversible: synthesis of fresh enzyme is required for
return of activity. Thus, the subject’s resolve not to drink is reinforced by
the distressing symptoms that occur if he drinks a little bit. It should not be
used in patients who are physically dependent on alcohol.
Side effects of disulfiram (as such) are infrequent, include
rashes, metallic taste, nervousness, malaise and abdominal upset. It inhibits a
number of other enzymes as well including alcohol dehydrogenase, dopamine β hydroxylase and
several cytochrome P450 isoenzymes. Thus, it prolongs t½ of many drugs.
Related Topics
