Dietary Fats
| Home | | Biochemistry |Chapter: Biochemistry : Nutrition
The incidence of a number of chronic diseases is significantly influenced by the kinds and amounts of nutrients consumed.
DIETARY FATS
The incidence of a
number of chronic diseases is significantly influenced by the kinds and amounts
of nutrients consumed (Figure 27.8 ). Dietary fats most strongly influence the
incidence of coronary heart disease (CHD), but evidence linking dietary fat and
the risk for cancer or obesity is much weaker.
Although earlier recommendations emphasized
decreasing the total amount of fat and cholesterol in the diet, data now show
that the type of fat is a more important risk factor than the total amount of
fat consumed.
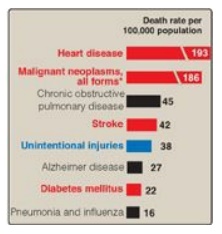
Figure 27.8 Influence of nutrition on some common causes of death in the United States in the year 2010. Red indicates causes of death in which the diet plays a significant role. Blue indicates causes of death in which excessive alcohol consumption plays a part. (*Diet plays a role in only some forms of cancer.)
A. Plasma lipids and coronary heart disease
Plasma cholesterol may
arise from the diet or from endogenous biosynthesis. In either case,
cholesterol is transported between the tissues in combination with protein and
phospholipids as lipoproteins.
1. Low-density lipoprotein and high-density lipoprotein: The level of plasma cholesterol is not precisely regulated but, rather, varies in response to the diet. Elevated levels of total cholesterol (hypercholesterolemia) result in an increased risk for CHD (Figure 27.9). A much stronger correlation exists between CHD and the level of cholesterol in low-density lipoproteins ([LDL-C]). As LDL-C increases, CHD increases. In contrast, high levels of high-density lipoprotein cholesterol (HDL-C) have been associated with a decreased risk for heart disease. [Note: Elevated plasma triacylglycerol (TAG) is associated with CHD, but a causative relationship has yet to be demonstrated.] Abnormal levels of plasma lipids (dyslipidemias) act in combination with smoking, obesity, sedentary lifestyle, insulin resistance, and other risk factors to increase the risk of CHD.
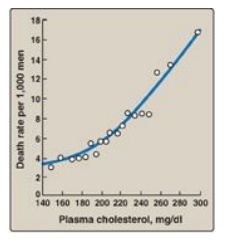
Figure 27.9 Correlation of the death rate from coronary heart disease with the concentration of plasma cholesterol. [Note: The data were obtained from a 6-year study of men with the death rate adjusted for age.]
2. Benefits of lowering plasma cholesterol: Dietary or drug treatment of hypercholesterolemia has been shown to be effective in decreasing LDL-C, increasing HDL-C, and reducing the risk for cardiovascular events. The diet-induced changes of plasma lipoprotein concentrations are modest, typically 10%–20%, whereas treatment with “statin” drugs decreases plasma cholesterol by 30%–60%. [Note: Dietary and drug treatment can lower TAGs.]
B. Dietary fats and plasma lipids
TAGs are quantitatively
the most important class of dietary fats. The influence of TAGs on blood lipids
is determined by the chemical nature of their constituent fatty acids. The
absence or presence and number of double bonds (saturated versus mono- and
polyunsaturated), the location of the double bonds (w-6 versus w-3), and the
cis versus trans configuration of the unsaturated fatty acids are the most
important structural features that influence blood lipids.
1. Saturated fat: TAGs composed primarily of fatty
acids whose hydrocarbon chains do not contain any double bonds are referred to
as saturated fats. Consumption of saturated fats is positively associated with
high levels of total plasma cholesterol and LDL-C and an increased risk of CHD.
The main sources of saturated fatty acids are dairy and meat products and some
vegetable oils, such as coconut and palm oils (a major source of fat in Latin
America and Asia, although not in the United States; Figure 27.10 ). Most
experts strongly advise limiting intake of saturated fats to less than 10% of
total caloric intake.
Saturated fatty acids with carbon chain lengths of
14 (myristic) and 16 (palmitic) are most potent in increasing the serum
cholesterol. Stearic acid (18 carbons, found in many foods including chocolate)
has little effect on blood cholesterol.
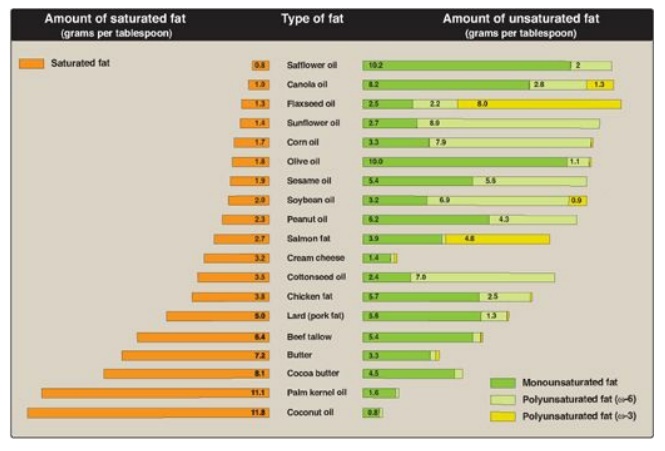
Figure 27.10 Compositions of commonly encountered dietary fats.
2. Monounsaturated fats: TAGs containing primarily fatty acids with one double bond are referred to as monounsaturated fat. Unsaturated fatty acids are generally derived from vegetables and fish. When substituted for saturated fatty acids in the diet, monounsaturated fats lower both total plasma cholesterol and LDL-C but maintain or increase HDL-C. This ability of monounsaturated fats to favorably modify lipoprotein levels may explain, in part, the observation that Mediterranean cultures, with diets rich in olive oil (high in monounsaturated oleic acid), show a low incidence of CHD. It is recommended that monounsaturated fats account for about 50% of the total fat intake.
a. The Mediterranean diet: The Mediterranean diet is an
example of a diet rich in monounsaturated fatty acids, or MUFAs (from olive
oil), and polyunsaturated fatty acids, or PUFAs (from fish oils and some nuts),
but low in saturated fat. For example, Figure 27.11 shows the composition of
the Mediterranean diet in comparison with both a Western diet similar to that
consumed in the United States and a typical low-fat diet. The Mediterranean
diet contains seasonally fresh food, with an abundance of plant material, low amounts
of red meat, and olive oil as the principal source of fat. The Mediterranean
diet is associated with decreased serum total cholesterol and LDL-C, decreased
TAGs, and increased HDL-C when compared with a typical Western diet higher in
saturated fats.
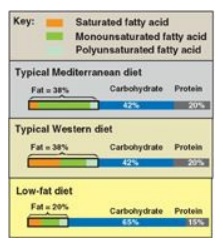
Figure 27.11 Composition of typical Mediterranean, Western, and low-fat diets.
3. Polyunsaturated fats: TAGs containing primarily fatty acids with more than one double bond are referred to as polyunsaturated fats. The effects of PUFAs on cardiovascular disease is influenced by the location of the double bonds within the molecule.
a. ω-6 Fatty acids: These are long-chain PUFAs, with
the first double bond the sixth bond position when starting from the methyl (ω)
end of molecule. [Note: They are also called n-6 fatty acids.]
Consumption of fats
containing w-6 PUFAs, principally linoleic acid (18:2 [9,12]), obtained from
vegetable oils, lowers plasma cholesterol when substituted for saturated fats.
Plasma LDL-C is lowered, but HDL-C, which protects against CHD, is also
lowered. The powerful benefits of lowering LDLs are only partially offset
because of the decreased HDL. Nuts, avocados, olives, soybeans, and various
oils, including sunflower, cottonseed, and corn oil, are common sources of
these fatty acids (see Figure 27.10 ). The AMDR for linoleic acid is 5%–10%.
[Note: The lower recommendation for PUFAs relative to MUFAs is because of
concern that free radical– mediated oxidation (peroxidation) of PUFAs may lead
to deleterious products.]
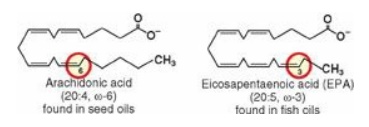
b. ω-3 Fatty acids: These are long-chain PUFAs, with
the first double bond beginning at the third bond position from the methyl (ω)
end. Dietary w-3 PUFAs suppress cardiac arrhythmias, reduce serum TAGs,
decrease the tendency for thrombosis, lower blood pressure, and substantially
reduce risk of cardiovascular mortality (Figure 27.12 ), but they have little
effect on LDL-C or HDL-C levels. Evidence suggests that they have
anti-inflammatory effects. The w-3 PUFAs, principally α-linolenic acid,
18:3(9,12,15), are found in plant oils, such as flaxseed and canola, and some
nuts. The AMDR for α-linolenic acid is 0.6%–1.2%. Fish oil contains the
long-chain ω-3 docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA). Two
fatty fish (for example, salmon) meals per week are recommended. For patients
with documented CHD, 1 g/day of fish oils is recommended, while 2–4 g/day is
prescribed to lower TAGs. [Note: The ω-3 long-chain PUFAs are included in
infant formulas to promote brain development.] Linoleic and α-linolenic acids
are essential fatty acids (EFAs) required for membrane fluidity and synthesis
of eicosanoids. EFA deficiency is characterized by scaly dermatitis as a result
of the depletion of skin ceramides with long-chain fatty acids.]
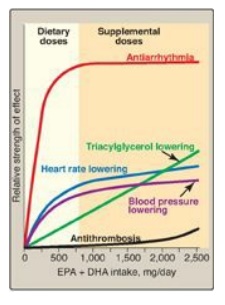
Figure 27.12 Dose responses of
physiologic effects of fish oil intake. EPA = eicosapentaenoic acid; DHA =
docosahexaenoic acid.
4. Trans fatty acids: Trans fatty acids ( Figure 27.13 )
are chemically classified as unsaturated fatty acids but behave more like
saturated fatty acids in the body because they elevate serum LDL-C (but not
HDL-C), and they increase the risk of CHD. Trans fatty acids do not occur
naturally in plants but occur in small amounts in animals. However, trans fatty
acids are formed during the hydrogenation of liquid vegetable oils (for
example, in the manufacture of margarine and partially hydrogenated vegetable
oil). Trans fatty acids are a major component of many commercial baked goods,
such as cookies and cakes, and most deep-fried foods. Many manufacturers have
reformulated their products to be free of trans fats. Starting in 2006, the
U.S. Food and Drug Administration requires that Nutrition Facts labels portray
the trans fat content of packaged food. Some municipalities, such as New York
City, have banned the use of trans fats in restaurants.
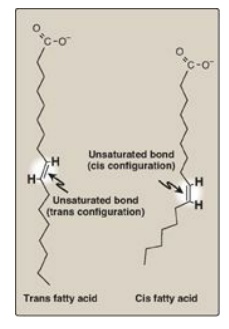
Figure 27.13 Structure of cis and trans fatty acids.
5. Dietary cholesterol: Cholesterol is found only in animal products. The effect of dietary cholesterol on plasma cholesterol (Figure 27.14 ) is less important than the amount and types of fatty acids consumed. Cholesterol consumption should be no more than 300 mg/day.
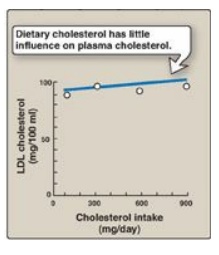
Figure 27.14 Response of plasma low-density lipoprotein (LDL) concentrations to an increase in dietary cholesterol intake.
C. Other dietary factors affecting coronary heart disease
Moderate consumption of
alcohol (up to 1 drink a day for women and up to 2 drinks a day for men)
decreases the risk of CHD, because there is a positive correlation between
moderate alcohol consumption and the plasma concentration of HDL-C. However,
because of the potential dangers of alcohol abuse, health professionals are
reluctant to recommend increased alcohol consumption to their patients. Red
wine may provide cardioprotective benefits in addition to those resulting from
its alcohol content (for example, red wine contains phenolic compounds that
inhibit lipoprotein oxidation;). [Note: These antioxidants are also present in
raisins and grape juice.] Figure 27.15 summarizes the effects of dietary fats.
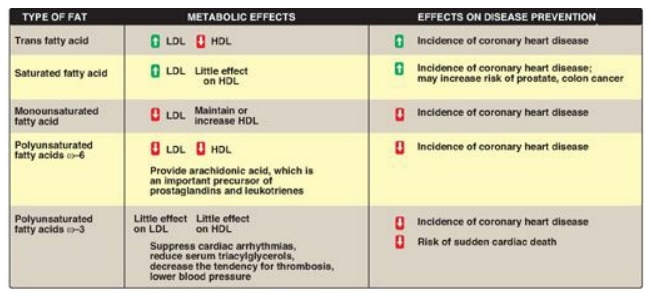
Figure 27.15 Effects of
dietary fats. LDL = low-density lipoprotein; HDL = high-density lipoprotein.
Related Topics
