Components of Antimicrobial Stewardship Programmes
| Home | | Pharmaceutical Microbiology | | Pharmaceutical Microbiology |Chapter: Pharmaceutical Microbiology : Antibiotic Prescribing And Antibiotic Stewardship
There are no nationally or internationally accepted guidelines on the structure of a stewardship programme, so they vary from country to country and even from one hospital to another within a geographical region. Indeed, even the titles vary, so terms like ‘good antimicrobial practice programmes’, ‘antibiotic management programmes’ and ‘antibiotic control programmes’ have all been used.
COMPONENTS OF ANTIMICROBIAL STEWARDSHIP PROGRAMMES
There are no nationally or internationally accepted guidelines on the
structure of a stewardship programme, so they vary from country to country and
even from one hospital to another within a geographical region. Indeed, even
the titles vary, so terms like ‘good antimicrobial practice programmes’,
‘antibiotic management programmes’ and ‘antibiotic control programmes’ have all
been used. There is, however, a measure of agreement on the personnel
comprising an antimicrobial stewardship team. They are multidisciplinary and
usually consist of:
• An infectious diseases physician
• An clinical pharmacist with infectious diseases training
• A medical microbiologist
• An infection control professional
• A hospital epidemiologist
• An information technology specialist.
In the USA the IDSA and the Society for
Heathcare Epidemiology of America (SHEA) set forth stewardship guidelines in
2007 that have been widely adopted both in the USA and elsewhere; but in Europe
the situation is less uniform. Here, an expert group reported in 2000 that
little was known about which stewardship measures were employed in Europe and
which were optimal. As a consequence, the European Commission Concerted Action
Antibiotic Resistance Prevention and Control (ARPAC) survey of stewardship
practices in 263 hospitals through 32 European countries was undertaken, and it
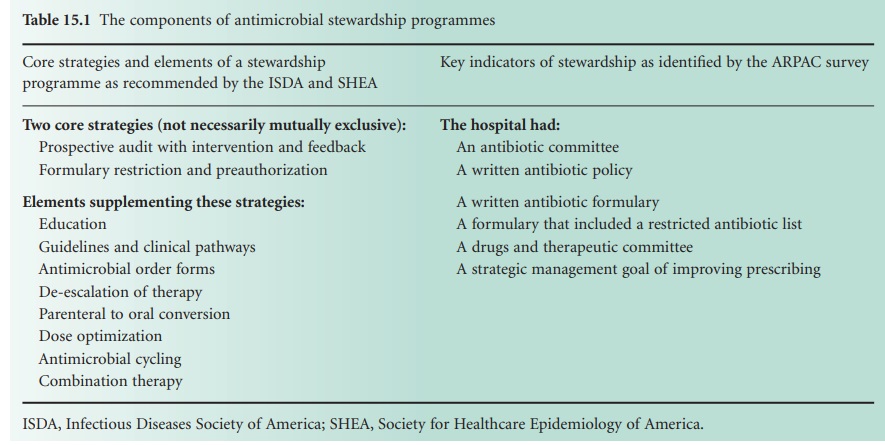
reported in 2009.Table 15.1 lists
both the components of the USguidelines and the six key indicators of
stewardship that were the subject of the ARPAC survey.
Before considering in more detail the elements
of a stewardship programme, it is worth explaining the meaning of some of the
terms used in Table 15.1. In
this context a prospective audit means a review of the future delivery of
healthcare to ensure that best practice is being carried out, so a prospective
audit with intervention and feedback is a process in which the use of
antibiotics is monitored and suggestions made for improvement, where necessary,
while the course of treatment is still in progress. The
feedback element is the provision of information to the prescriber about the
drug in question, e.g. local resistance patterns and dose information based
upon pharmacokinetic data.
Most hospitals have a drugs and
therapeutics committee (DTC; sometimes also known as a pharmacy and
therapeutics committee) whose function is to evaluate drugs for inclusion in a
hospital formulary on the basis of their efficacy, toxicity and cost. The
intention is to avoid the unnecessary stocking of multiple drugs from the same
class which have similar or identical properties; few hospitals stock every
available aminoglycoside or third generation cephalosporin, for example. An
antibiotics committee would be a subgroup of the DTC with responsibility for
selecting the drugs for inclusion in the antibiotics formulary. The strategy of
formulary restriction and preauthorization could limit the availability of
certain antibiotics simply by excluding them from the formulary (although they
could usually be obtained in exceptional circumstances if required). The
preauthorization element would simply be a requirement to seek the recommendation
(or even written approval) of senior clinical staff when prescribing antibiotics
in a restricted category—usually those drugs whose effectiveness needs to be preserved
because of their value in treating infections for which few drugs are
effective, e.g. linezolid or daptomycin, or antibiotics which may predispose to
other problems, e.g. clindamycin because of its link to Clostridium difficile outbreaks.
The ARPAC stewardship indicator that the hospital should have a
strategic management goal of improving prescribing has important implications
for the provision of resources and granting the authority to implement
decisions. Establishing a stewardship programme costs money: staff time must be
available for (1) the preparation of the antibiotics policy document and
formulary, (2) intervention and feedback, and (3) monitoring of antibiotic use
and resistance patterns. It is easier to gain approval for the necessary budget
allocation if there is a publically stated management goal of improving
prescribing. Where pre-authorization for selected antibiotics is a part of the
programme, the greater the authority bestowed on the person(s) making the
recommendations, the greater the effectiveness of the policy has been shown to
be.
Related Topics
