Centrally Acting Muscle Relaxants
| Home | | Pharmacology |Chapter: Essential pharmacology : Skeletal Muscle Relaxants
These are drugs which reduce skeletal muscle tone by a selective action in the cerebrospinal axis, without altering consciousness. They selectively depress spinal and supraspinal polysynaptic reflexes involved in the regulation of muscle tone without significantly affecting monosynaptically mediated stretch reflex.
CENTRALLY ACTING MUSCLE RELAXANTS
These are drugs which
reduce skeletal muscle tone by a selective action in the cerebrospinal axis,
without altering consciousness. They selectively depress spinal and supraspinal
polysynaptic reflexes involved in the regulation of muscle tone without significantly
affecting monosynaptically mediated stretch reflex. Polysynaptic pathways in
the ascending reticular formation which are involved in the maintenance of
wakefullness are also depressed, though to a lesser extent. All centrally
acting muscle relaxants do have some sedative property. They have no effect on
neuromuscular transmission and on muscle fibres, but reduce decerebrate
rigidity, upper motor neurone spasticity and hyperreflexia.
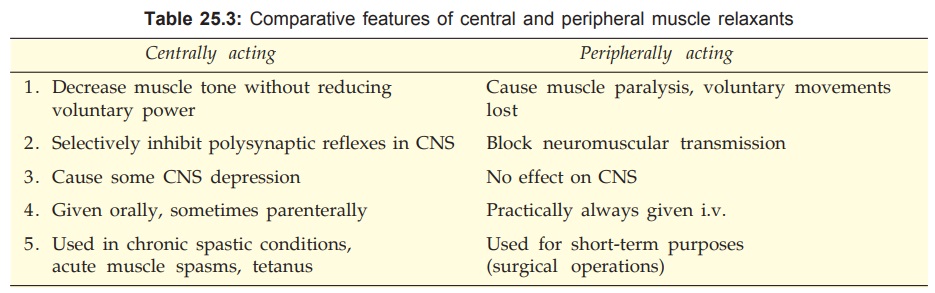
The prominent
differences between peripherally and centrally acting muscle relaxants are
listed in Table 25.3.
CLASSIFICATION
(i) Mephenesin congeners
Carisoprodol,
Mephenesin,
Chlorzoxazone,
Chlormezanone,
Methocarbamol.
(ii) Benzodiazepines
Diazepam and others.
(iii) GABA
derivative
Baclofen.
(iv) Central α2 agonist
Tizanidine
Mephenesin
It was the first drug
found to cause muscle relaxation in
animals without producing unconsciousness and was called internuncial neurone blocking agent because its primary site of
action is the spinal internuncial neurone which modulates reflexes maintaining
muscle tone. It is not used clinically because it is gastric irritant, and injected
i.v., it causes thrombophlebitis, haemolysis and marked fall in BP. It has been
included in counterirritant ointments (MEDICREME,
RELAXYL) where its irritant rather than muscle relaxant property could
be affording relief.
Carisoprodol
It has a favourable
muscle relaxant: sedative
activity ratio with weak analgesic, antipyretic and anticholinergic actions in
addition. It is used in musculoskeletal disorders associated with muscle spasm.
CARISOMA 350 mg tab; one tab. TDSQID, SOMAFLAM 175 mg +
ibuprofen 400 mg tab.
Chlorzoxazone
It is
pharmacologically similar to mephenesin;
has a longer duration of action and is better tolerated orally.
PARAFON DSC 500 mg
tab; MOBIZOX 500 mg + diclofenac 50 mg + paracetamol 500 mg tab; PARAFON: 250
mg + paracetamol 300 mg tab, 1–2 tab TDS.
Chlormezanone
It has antianxiety and
hypnotic actions as well, and has been used for tension states associated with
increased muscle tone.
WINTRAC 100 mg tab; 1–2 tab TDSQID, DOLOBAK 100 mg +
paracetamol 450 mg tab.
Methocarbamol
It is less sedative
and longer acting than
mephenesin. Orally it has been used in reflex muscle
spasms and chronic neurological diseases. It can be injected i.v. without
producing thrombophlebitis and haemolysis— used for orthopedic procedures and
tetanus.
ROBINAX 0.5 g tab, 1 TDS: 100 mg/ml inj. for i.v. or i.m. use.
ROBIFLAM 750 mg + ibuprofen 200 mg tab;
FLEXINOL 400 mg + paracetamol
325 mg tab.
Clinical efficacy of none of the above drugs as muscle relaxant
is well established. Gastric irritation and sedation are the most important
side effects.
Diazepam
It is the prototype of benzodiazepines (BZDs)
which act in the brain on specific receptors enhancing GABAergic transmission.
Muscle tone is reduced by supraspinal rather than spinal action; muscle
relaxant: sedative activity ratio is low. No gastric irritation occurs and it
is very well tolerated, though sedation limits the dose which can be used for
reducing muscle tone. It is particularly valuable in spinal injuries and
tetanus. Combined with analgesics, it is popular for rheumatic disorders
associated with muscle spasm.
Dose: 5 mg TDS orally, 10–40
mg i.v. (in tetanus).
Baclofen
This analogue of the
inhibitory transmitter GABA acts
as a selective GABAB receptor agonist. The GABA receptors have been
divided into:
GABAA receptor Intrinsic ion channel
receptor— increases Cl¯
conductance; blocked by bicuculline; facilitated by BZDs.
GABAB receptor Gprotein coupled
receptor; hyperpolarizes
neurones by increasing K+ conductance and altering Ca2+
flux; bicuculline insensitive; blocked by saclofen.
Baclofen does not affect Cl¯ conductance and its actions are not
antagonized by bicuculline.
The primary site of
action of baclofen is considered to be in the spinal cord where it depresses
both polysynaptic and monosynaptic reflexes. As such, it does produce muscle
weakness, but is less sedative than diazepam. It reduces spasticity in many
neurological disorders like multiple sclerosis, amyotropic lateral sclerosis,
spinal injuries and flexor spasms, but is relatively ineffective in stroke,
cerebral palsy, rheumatic and traumatic muscle spasms and parkinsonism.
Baclofen is well absorbed
orally and is primarily excreted unchanged in urine with a t½ of 3–4 hours.
Side Effects are drowsiness, mental confusion, weakness and ataxia; serum
transaminases may rise. Sudden withdrawal after chronic use may cause hallucinations,
tachycardia and seizures.
Dose: 10 mg BD to 25 mg TDS.
LIORESAL, LIOFEN 10
mg, 25 mg tab.
Tizanidine
This recently
introduced clonidine congener is a central α2 adrenergic
agonist—inhibits release of excitatory amino acids in the spinal inter-neurones.
It may facilitate the inhibitory transmitter glycine as well. It inhibits
polysynaptic reflexes; reduces muscle tone and frequency of muscle spasms
without reducing muscle strength. Efficacy similar to baclofen or diazepam has
been noted in multiple sclerosis, spinal injury and stroke, with fewer side
effects.
Tizanidine is absorbed
orally, undergoes first pass metabolism and is excreted by the kidney; t½ 2–3
hours. It is indicated in spasticity due to neurological disorders and in painful
muscle spasms of spinal origin. Side effects are dry mouth, drowsiness, nighttime
insomnia and hallucinations. Dose-dependent elevation of liver test values has
been noted. Though no consistent effect on BP has been observed, it should be
avoided in patients receiving antihypertensives, especially clonidine.
Dose: 2 mg TDS; max 24
mg/day.
SIRDALUD 2 mg tab,
TIZAN 2, 4 mg tab; TIZAFEN 2 mg + ibuprofen 400 mg tab; TIZANAC 2 mg + diclofenac
50 mg tab, PROXIVONMR 2 mg + nimesulide 100 mg cap.
Uses Of Centrally Acting Muscle Relaxants
1. Acute Muscle
Spasms
Overstretching of a muscle, sprain, tearing of ligaments and
tendons, dislocation, fibrositis, bursitis, rheumatic disorders, etc. cause
painful spasm of muscles. The mephenesin like and BZD muscle relaxants,
combined with analgesics, are commonly used, but efficacy is not impressive.
2. Torticollis,
Lumbago, Backache, Neuralgias
These are other conditions in which painful spasm of certain
muscles is a prominent feature; respond in the same way as acute muscle spasms.
3. Anxiety And Tension
These states are often associated with increased tone of muscles.
Diazepam group of drugs and chlormezanone benefit by their antianxiety as well as
muscle relaxant actions.
4. Spastic Neurological Diseases
Impairment of descending pathways
in the cerebrospinal axis and withdrawal of inhibitory influence over the
stretch reflex causes chronic increase in muscle tone or spasticity.
Hemiplegia, paraplegia, spinal injuries, multiple sclerosis, amyotropic lateral
sclerosis and cerebral palsy fall in this category. They are benefited by
baclofen, diazepam, tizanidine and dantrolene but not by mephenesin group of
drugs. However, therapy of these disorders is far from satisfactory.
5. Tetanus
Most commonly diazepam
is infused i.v. and the dose is titrated by the response. Methocarbamol is an
alternative.
6. Electroconvulsive Therapy
Diazepam decreases the
intensity of convulsions resulting from ECT, without diminishing its
therapeutic effect. Often SCh is used in addition for total suppression of the
muscular component of ECT.
7. Orthopedic Manipulations
These may be performed under the influence of diazepam or
methocarbamol given i.v.
Related Topics
