Axial Skeleton
| Home | | Anatomy and Physiology | | Anatomy and Physiology Health Education (APHE) |Chapter: Anatomy and Physiology for Health Professionals: Support and Movement: Bone Tissues and the Skeletal System
1. Compare the axial skeleton with the appendicular skeleton. 2. Explain the bones of the cranium. 3. List the facial bones. 4. Compare the mandible with the hyoid bone. 1. List the numbers of cervical, thoracic, and lumbar vertebrae. 2. Explain the structure of the sternum. 3. Distinguish between true, false, and floating ribs.
Axial
Skeleton
Skeletal
Organization
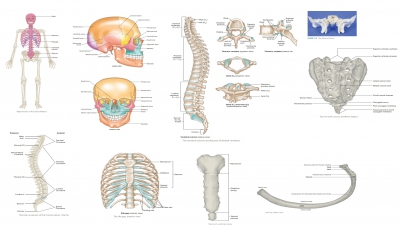
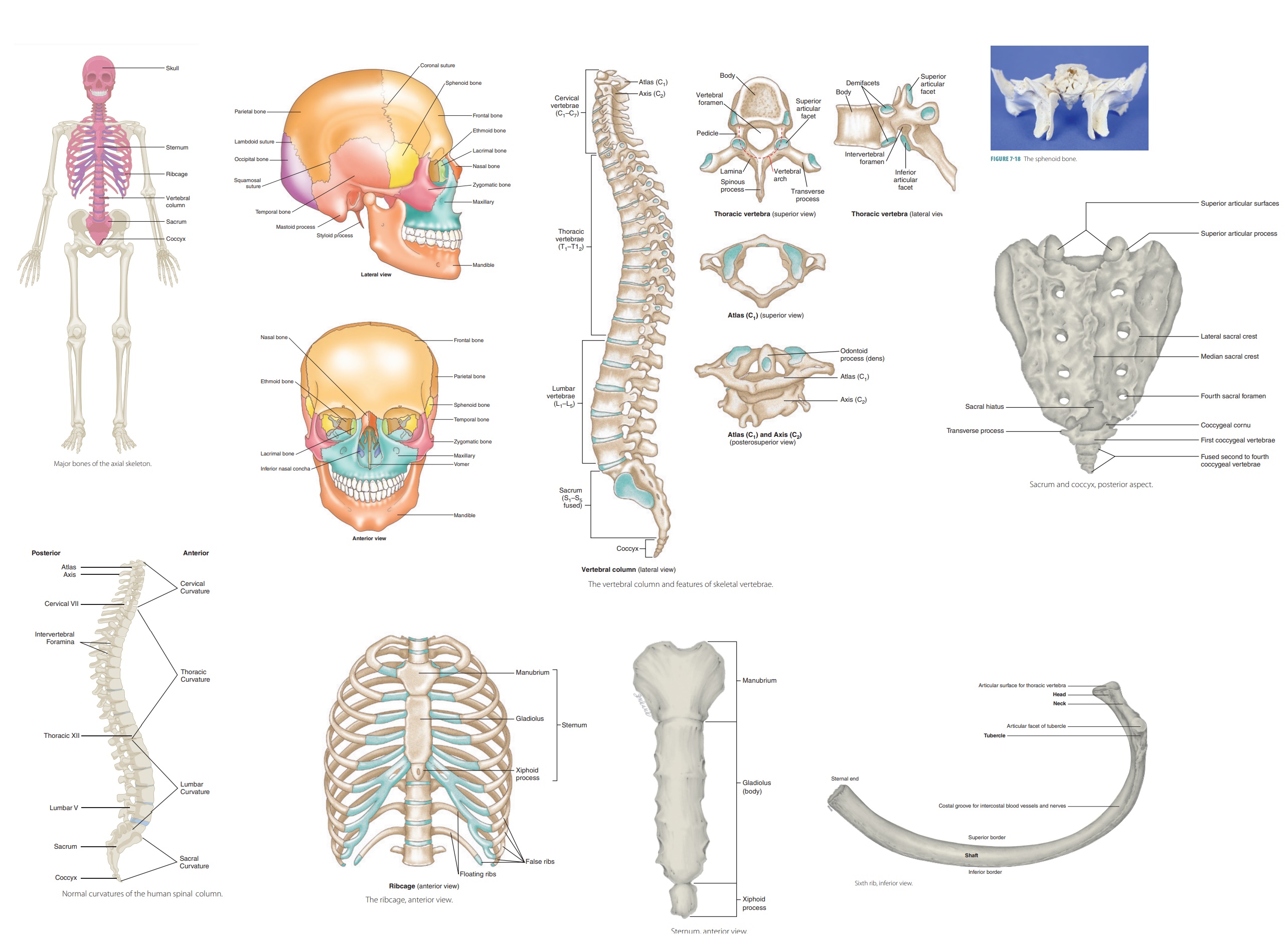
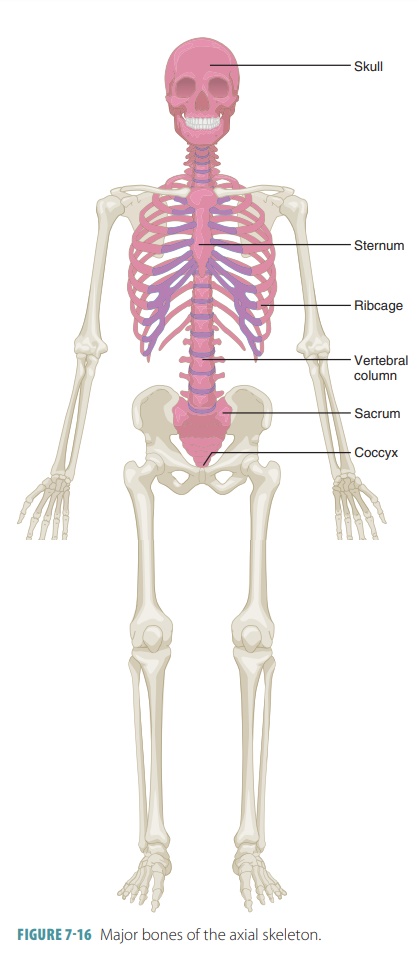
The skeleton is divided into two
major portions: the axial skeleton (FIGURE 7-16 ) and the appendicular skeleton. Including those of the middle ear,
there are 206 bones in the human body.
Axial
Skeleton
The axial skeleton supports and
protects the head, neck, and trunk. It includes the skull, hyoid bone (a
single bone in the neck that supports the tongue and its muscles), vertebral
column, and thoracic cage.
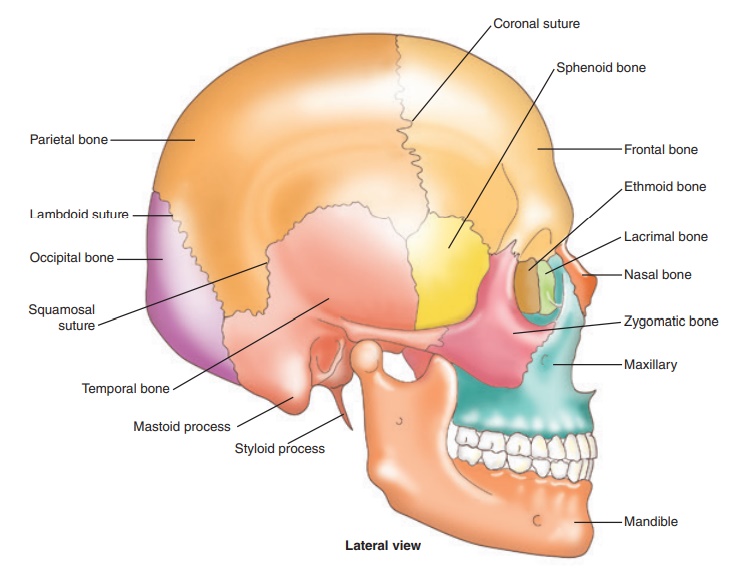
Skull
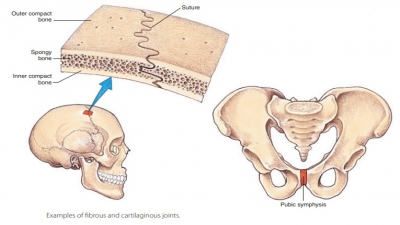
The human skull is made up of 22 firmly
interlocked bones. These are divided into the cranium and the facial bones. The cranium is made up of eight bones and the
face is made up of 14. The lines where the bones of the skull lock together are
called sutures. The only movable bone in the skull is the mandible (lower jaw), which is attached to the cranium by ligaments. The
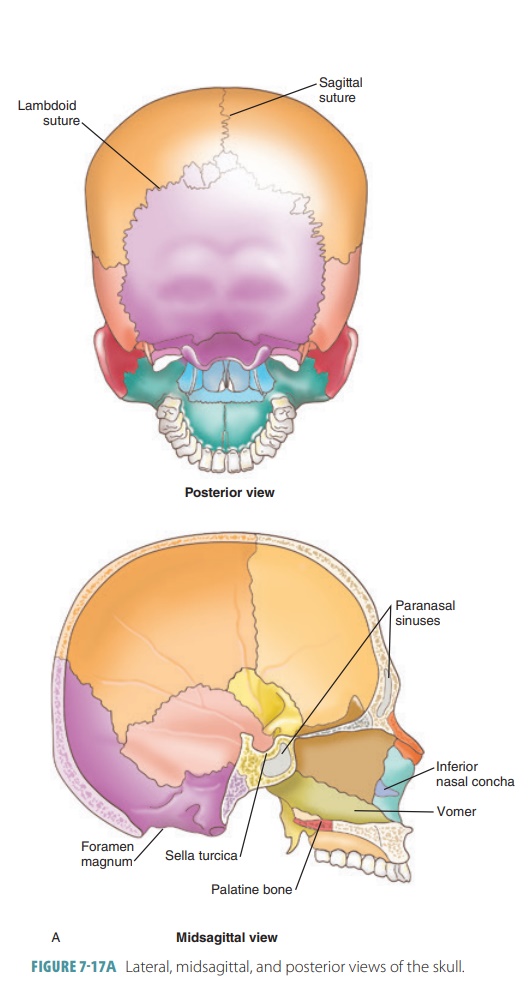
cranium houses and protects the brain. Air-filled spaces inside the cranial
bones called paranasal sinuses help
the voice to resonate and also reduce the weight of the skull. The cranial
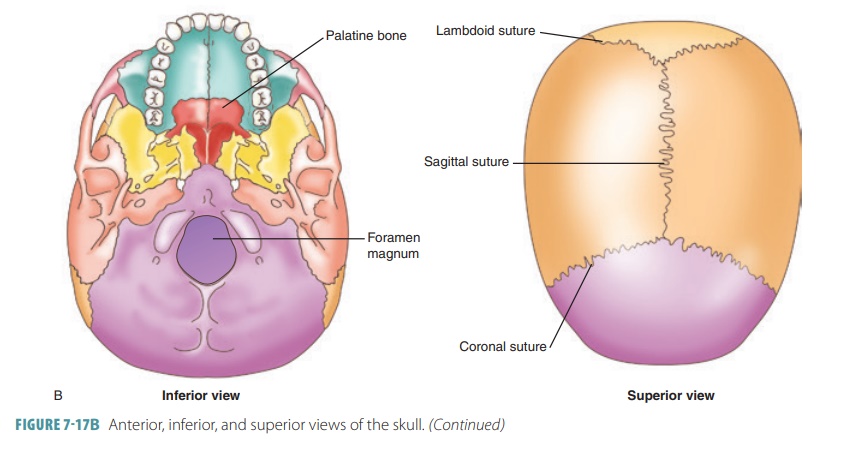
bones enclose the chamber that supports the brain, which is known as the cranial cavity. FIGURES 7-17A and 7-17B show various views of the human
skull and its bones.
Cranium
The cranium consists of eight
bones
■■ Frontal bone: This bone forms
the anterior skull above the eyes, with each eye orbit (the eye socket) aving a
supraorbital foramen (notch). Blood vessels and nerves pass through this
structure to the forehead tissues. The frontal bone contains two frontal
sinuses above the central part of the eyes. The frontal squama is also known as
the forehead, forming the anterior, superior portion of the cranium. It
provides a surface area where the facial muscles attach. The lacrimal fossa is
a shallow depression marking the location of the lacrimal (tear) gland.
■■ Parietal bones: Located on
each side of the skull behind the frontal bone, these two bones form the sides
and roof of the cranium and are fused in the middle along the sagittal suture.
They meet the frontal bone along the coronal suture.
■■ Occipital bone: Joining the
parietal bones along the lambdoid suture, the occipital bone forms the back of
the skull and base of the cranium. A large opening at the lower portion of this
bone (the foramen magnum) allows nerve fibers to pass through from the brain into
the spinal cord. The jugular foramen is between the occipital and temporal
bones and allows the internal jugular vein to pass through. Rounded occipital
condyles on each side of the foramen magnum articulate with the first vertebra
of the spine. The hypoglossal canals begin at each occipital condyle’s lateral
base, ending on the inner surface of the occipital bone near the foramen
magnum. The hypoglossal nerves pass through them. The external occipital
protuberance is a small bump on the inferior surface, at the midline, of the
occipital bone. The external occipital crest begins here, marking the
attachment of a ligament that helps stabilize the neck vertebrae.
■■ Temporal bones: These two
bones join the parietal bone on each side of the skull along the squamous
suture, and form parts of the sides and base of the cranium. An opening called
the external acoustic meatus leads through each temporal bone to the inner ear.
The mandibular fossae are depressions that articulate with the mandible. Two
projections below each external acoustic meatus (the mastoid process and the
styloid process) provide points of attachment. The mastoid process attaches to
certain neck muscles, and the styloid process attaches to muscles of the tongue
and pharynx. The zygomatic process projects from the temporal bone to join the
zygomatic bone, helping to form the cheek at the zygomatic arch. The squamous
part of the temporal bone is convex and irregular, bordering the squamous
suture. The petrous part of the temporal bone encloses the structures of the
inner ear. The auditory ossicles are located inside the tympanic cavity (middle
ear). They transfer sound vibrations from the eardrum to the inner ear. The
carotid canal provides a passageway for the internal carotid artery of the
brain. The foramen lacerum is thin, extending between the sphenoid and temporal
bones, containing hyaline cartilage and small arteries supplying the inner
surface of the cranium. The stylomastoid foramen is posterior to the base of
the styloid process, allowing the facial nerve to pass through. The internal
acoustic meatus is a canal that carries blood vessels and nerves to the inner
ear as well as the facial nerve to the stylomastoid foramen.
■■ Sphenoid bone: This complex,
bat-shaped bone forms part of the base of the cranium, sides of the skull, and
floors and sides of the eye orbits (FIGURE 7-18). The eye orbits are actually
formed by seven bones in total, known as the orbital complexes. Each orbital
complex consists of portions of the sphenoid, frontal, maxilla, lacrimal,
ethmoid, palatine, and zygomatic bones. The superior portion of the sphenoid
bone has an indentation that forms the sella turcica (Turk’s saddle), which
contains the pituitary gland in its “seat”
known as the hypophyseal
fossa. It is considered the cranium’s keystone because it articulates with all
other cranial bones. The sphenoid bone is described as having a central body and three pairs of processes known as the greater wings, lesser wings, and pterygoid
processes. The body of the
sphenoid bone houses two sphenoidal
sinuses . The greater wings
project laterally from the body of the sphenoid bone. They form parts of the
middle cranial fossa, the posterior
orbit walls, and the external skull wall. At this final point, they are
flag-shaped, areas medial to the zygomatic arch. The sphenoid bone’s lesser wings resemble
horns and form part of the anterior cranial fossa’s floor as well as part of
the orbits’ medial walls. The pterygoid processes are narrow depressions,
projecting inferiorly from where the body and greater wings join. They anchor
the chewing- related pterygoid muscles.
The sphenoid bone has many openings. The optic
canals, anterior to the sella turcica,
allow the optic nerves to reach the eyes. A crescent- shaped row of four
open-ings lies on each side of the sphenoid body. The most anterior opening is
the superior orbital fissure, which appears as a long slit between the greater and lesser
wings. This fissure allows cra-nial nerves III, IV, and VI to enter the orbit.
It can be easily seen in an anterior skull view. Two other openings, the foramen rotundum and foramen ovale
, create passageways for cranial nerve V to reach the
face. The foramen rotundum is usually oval (not round) in shape, regardless of
its name. The large foramen ovale lies posterior to the foramen rotundum and is
also seen in an inferior view of the skull. The small foramen spi-nosum lies posterolateral to the foramen ovale and allows the middle meningeal artery to pass through, serving certain cranial
bones. The sphe-noid bone serves as a bridge uniting the cranial and facial
bones.

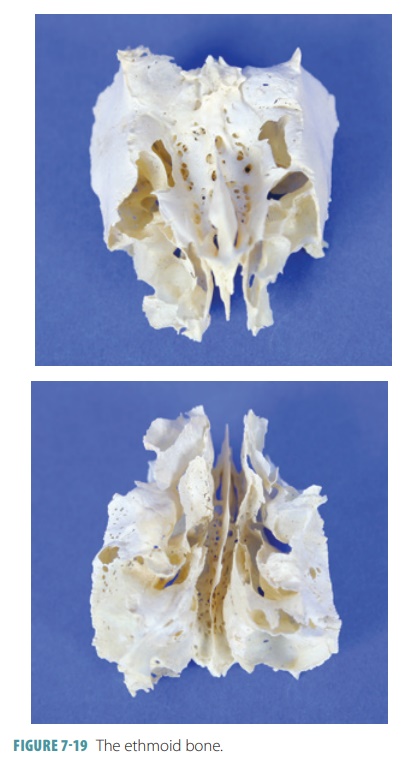
■■ Ethmoid
bone: Located in front of
the sphenoid
bone, the ethmoid
bone forms a mass on each side of the nasal cavity that is joined by thin cribriform plates that partially form the roof of the nasal cav-ity. Between
the cribriform plates, a triangular pro-cess (the crista
galli) attaches to
membranes that enclose the brain. Parts of the ethmoid bone form pieces of the cranial floor, walls of the eye orbits, and walls of the
nasal cavity. A perpendicular plate forms most of the nasal septum. The supe-rior nasal conchae and middle nasal conchae project inward toward the perpendicular plate,
with the lateral ethmoid bone containing many ethmoidal sinuses (FIGURE 7-19). The lateral masses
contain the ethmoidal
labyrinth, which has
interconnected ethmoidal air cells opening into the nasal cavity on either side. The olfactory
foramina inside the crib-riform plate allow passage of the olfactory
nerves.
Fontanels
In infants, the cranial bones are
connected by fibrous membranes through fontanels (soft spots) that allow the cranium to slightly change shape. When the
infant is born, the cranium compresses somewhat in order to pass through the
birth canal. The fontanels eventually close as the cranium ossifies and the
bones grow together. The skull of an infant fractures less easily than that of
an adult. The two fontanels are termed anterior
and posterior . The anterior
fon-tanel closes at 18 months of age and the posterior fontanel closes at two
months of age.
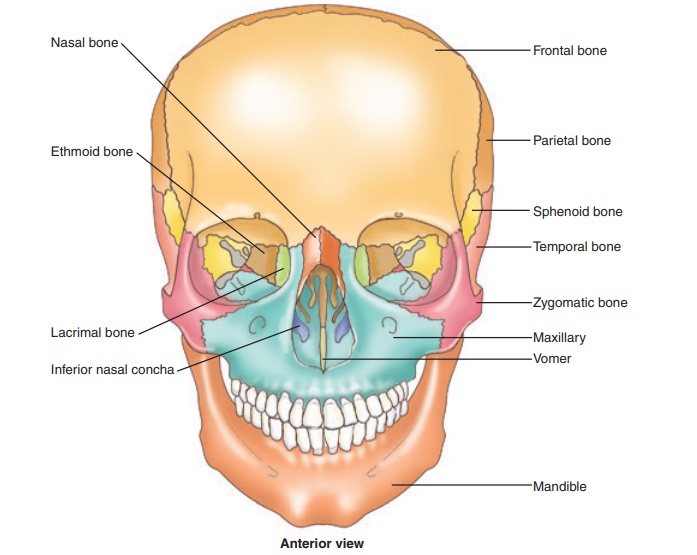
Facial Bones
The facial
skeleton consists of the following 14
bones (Figures 7-17A and 7-17B):
■■ Maxillae: These two bones form the upper jaw, anterior roof of the mouth (hard palate), floors of the eye orbits, and the nasal cavity sides and floor. The maxillae contain the upper teeth sockets as well as the maxillary sinuses, which are the largest sinuses in the skull. The orbital rim protects the eye and other structures in the eye orbit. As the human body grows, palatine processes of the maxillae grow together and fuse to form the anterior hard palate. Along with the alveolar process, the alveolar arch (dental arch) is formed, where the teeth are bound via dense connective tissue. The nasolacrimal canal is formed by a maxilla and lacrimal bone, protecting the lacrimal sac and nasolacrimal duct, through which tears flow from the orbit to the nasal cavity. The infraorbital foramen allows passage of a major sensory nerve reaching the brain through the foramen rotundum of the sphenoid bone. Between the maxillae and sphenoid, the inferior orbital fissure allows passage of blood vessels and cranial nerves.
■■ Zygomatic bones:
These two bones form the cheek prominences below the eyes as well as the
lateral walls and floors of the eye orbits. A temporal process extends from
the zygomatic bones to form a zygomatic arch. The zygomaticofacial foramen on
each zygomatic bone’s anterior surface allows passage of a sensory nerve that
innervates the cheek.
■■ Nasal bones: These
two long, thin bones lie side by side, fusing at the midline to form the bridge
of the nose. Flexible cartilages support the distal nose and extend along with
soft tissues to the superior bor-der of the external nares, which are the
entrances to the nasal cavity. The nasal complex consists of bones that enclose
the nasal cavities as well as the paranasal sinuses. These bones include the
fron-tal, sphenoid, ethmoid, maxilla, lacrimal, ethmoid, palatine, and inferior
nasal conchae.
■■ Vomer bone: This
thin, flat bone is found along the midline of the nasal cavity, joining the
ethmoid bone to form the nasal septum.
■■ Inferior nasal conchae:
These two bones are scroll-shaped, attached to the lateral nasal cavity walls,
and support the mucous membranes of the cavity.
■■ Lacrimal bones:
These two thin structures are located in the medial wall of each eye orbit
between the maxillae and ethmoid bone. A groove along the anterior lateral
surface, known as the lacrimal sulcus, marks the location of the lacrimal sac.
■■ Palatine bones:
Located behind the maxillae, the two L-shaped palatine bones form the posterior
hard palate and nasal cavity floor as well as the nasal cavity lateral walls.
The horizontal plate actually forms the posterior hard palate, whereas the
perpendicular plate extends from the horizontal plate to the orbital process,
forming part of the floor of the orbit.
■■ Mandible: This
horseshoe-shaped bone projects upward at each end with the mandibular condyle
and coronoid process. These processes are separated by the mandibular notch.
The mandible articulates with the temporal bone and provides attachments for
the muscles needed for chewing. The curved alveolar arch contains the hollow
sockets for the lower teeth. The mandible is the only movable bone of the
facial skeleton. The body of the mandible is its horizontal portion, whereas
the ramus is the ascending portion beginning at the mandibular angle on each
side. The mental foramina open to allow nerves to pass through that carry
sensory information from the lips and chin to the brain. The mandibular foramen
is where the mandibular canal begins, which allows blood vessels and nerves to
pass that service the lower teeth. The mandible articulates with the temporal
bone at the mandibular fossa.
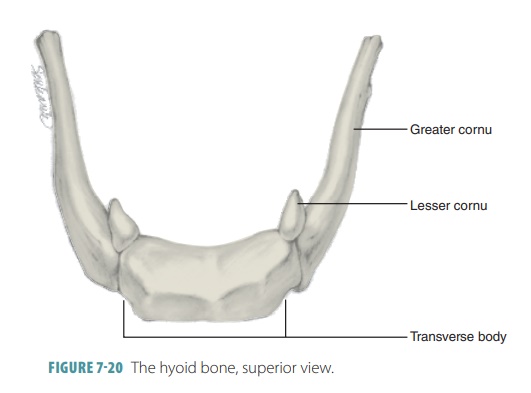
Hyoid Bone
The hyoid bone is unique in that
it is not actually part of the skull and lies just below the mandible in the
anterior neck. It actually resembles the man-dible in shape but is much smaller
(FIGURE 7-20). It is the only bone in the body that does not artic-ulate directly
with any other bone, but is instead anchored by thin stylohyoid ligaments to the sty-loid processes of the temporal
bones. Its somewhat “horseshoe” shape consists of a body and two pairs of cornua
(horns). The greater horns (cornua)
help to support the larynx and attach to the tongue muscles. The lesser cornua are attached to the
stylohyoid ligaments. The hyoid one is a movable base for the tongue, serving
to provide attachment points for neck muscles that control laryngeal movements
during speech and swallowing.
Spine
The vertical axis of the human
skeleton is formed by the vertebral
column (backbone), which extends from
the skull to the pelvis. It is made up of 26 bony vertebrae, separated by intervertebral discs made of cushioning
cartilage, connected by ligaments (FIGURE 7-21). Each
vertebra has a drum- shaped body, making up the thick anterior portion of the
bone.
The head and trunk are supported
by the vertebral column, which also protects the spinal cord. The spinal cord
passes through a vertebral canal
created by open-ings in the vertebrae. At the bottom of the backbone,some
vertebrae are fused to form the sacrum (a part of the pelvis) and the coccyx (tailbone), which is attached to the end of the sacrum.
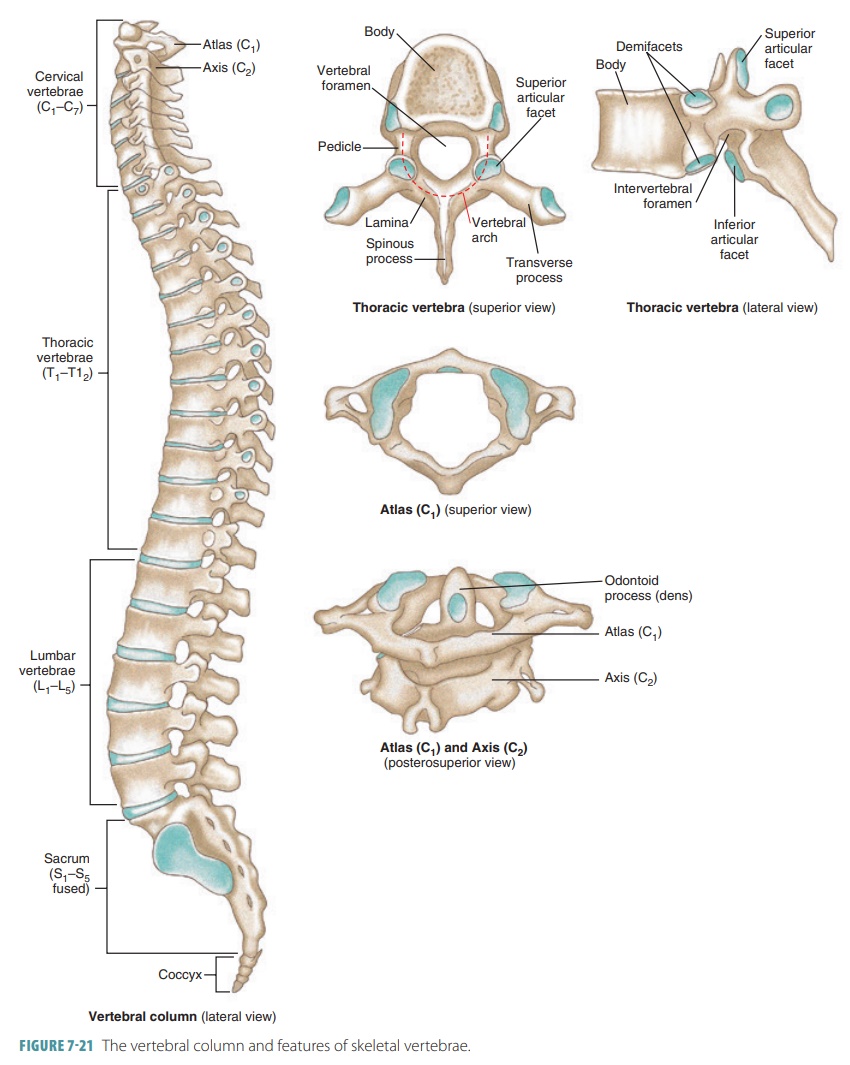
Vertebrae Structure
The vertebral body (centrum) is the area of a verte-bra that transfers
weight along the vertebral column’s axis. Two short stalks (pedicles) project
from each drum-shaped vertebra, with two plates called lam-inae that fuse to
become a spinous process. These structures collectively form a bony vertebral arch around the vertebral foramen, where the spinal cord passes through. A transverse process projects pos-teriorly, attached to ligaments and
muscles. Superior and inferior articular
processes project upward and downward with cartilage coverings, joined to
the ver-tebra above and below. Each articular process has a smooth concave
surface known as an articular facet.
Notches align with adjacent vertebrae forming open-ings (intervertebral foramina) through
which the spinal nerves pass.
Beginning with those located at
the top of the spine with the others listed sequentially (moving down the
spine), the vertebrae that make up the spine are:
■■ Cervical vertebrae: These
seven structures com-prise the neck, with distinctive transverse pro-cesses and
round transverse foramina, which allow the arteries leading to the brain to pass through. The
forked processes of the second through to the fifth cervical
vertebrae provide attachments for muscles.
The atlas (first vertebra supports the head with two kidney-shaped facets
articulating with the occipital condyles. It is dif-ferent from the other
vertebrae, because it lacks a body and spinous process and has a large, round
vertebral foramen that is bounded by anterior and posterior arches. The axis (second vertebra) has a process
(the dens) that projects upward into
the ring of the atlas. When the head turns side to side, the atlas pivots
around the dens. A notched spinous process, such as those on the C2
to C6 vertebrae, is referred to as bifid. The transverse processes are fused laterally to the costal processes, originating near the
ventrolateral portion of the vertebral body. A partial or complete dislocation
of the cervical vertebrae may result from sudden acceleration or deceleration,
such as in a car crash, causing an injury to the muscles, ligaments, and spinal
cord that is referred to as whiplash.
The last cervical vertebra (C7) resembles the first thoracic
vertebra (T1). This rule is generally true where each different
section of the vertebrae joins the next. C7, the vertebra prominens, has a
long, thin spinous process ending in a broad tubercle that can be felt through
the skin at the base of the neck. The ligamentum
nuchae is a thick elastic ligament
that begins at C7 and extends to insert along the skull’s occipital
crest.
■■ Thoracic vertebrae: These 12 structures are larger than the cervical vertebrae and have long processes that slope downward to articulate with the ribs. The thoracic vertebrae increase
in size down the spine to bear increasing loads of body weight. Each thoracic
vertebra articulates with ribs along the body’s dorsolateral surfaces. The costal facets on the vertebral bodies articulate
with the heads of the various ribs. The
transverse processes of vertebrae, T1 to T10, are
relatively thick. They contain transverse
costal facts for rib articulation.
■■ Lumbar
vertebrae: These five
structures in the lower back are even
larger than the thoracic ver-tebrae, supporting more body weight. The lum-bar
vertebrae do not have costal facts, but their slender transverse processes
project dorsolater-ally. They have a triangular vertebral foramen, with short
spinous processes projecting dorsally. The superior articular processes face
medially, whereas the inferior articular processes face laterally.
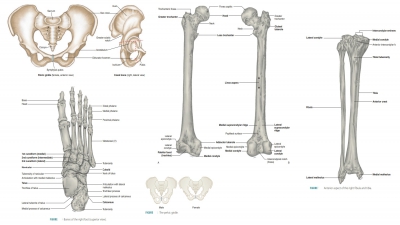
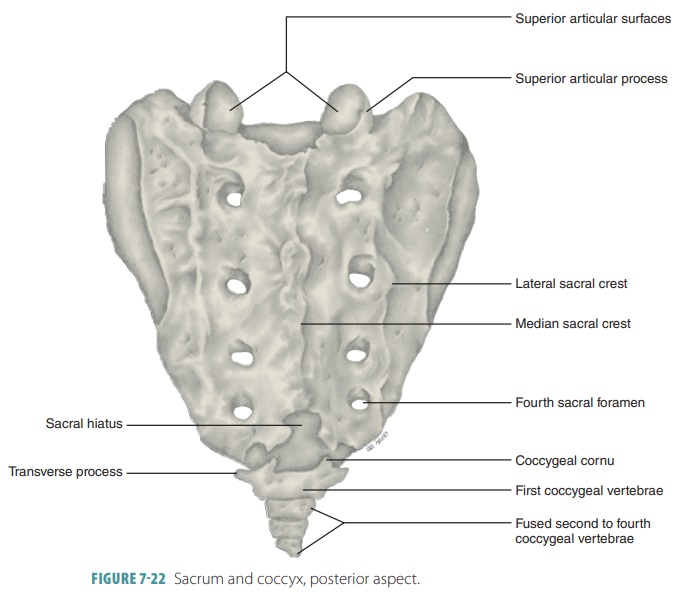
■■ Sacrum: This triangular structure
forms the posterior wall of the pelvis. It contains five fused vertebrae, S1
to S5, and forms the vertebral column’s base ( FIGURE 7-22). The
sacrum articulates superiorly via the superior
articular processes with L5
. It also articulates inferiorly with
the coccyx. Its auricular surfaces
are lat-erally articulated with the hip bones, forming the sacroiliac joints of the
pelvis. The sacral promontory is the anterosuperior margin of
the first sacral vertebra. It bulges
anteriorly into the pelvic cavity. Its body’s center of gravity lies
approximately 1 cm posterior to the sacral prom-ontory. Four transverse ridges cross the con-cave anterior aspect and mark lines of fusion of
the sacral vertebrae. The anterior sacral
foram-ina, at the lateral ends of the transverse ridges, transmit blood vessels and anterior
rami of the sacral spinal nerves.
Lateral to these foramina are expanded superior regions with a wing-like
appearance. They are called alae . The poste-rior midline sacral surface is made rough by
the fused spinous processes of the sacral vertebrae, which form the median sacral crest. Flank-ing this crest laterally are the posterior sacral foramina. These openings transmit the pos-terior rami of the sacral
spinal nerves and the lateral
sacral crests, which are remnants
of the transverse processes of S1 to S3.
The sacral canal continues through the sacrum to an exter-nal opening called
the sacral hiatus, where four pairs of anterior sacral foramina allow nerves
and blood vessels to pass. The sacral hiatus forms because the laminae of the
fifth and sometimes fourth sacral vertebrae do not fuse medially. The sacral
hiatus is located at the inferior end of the sacral canal.
■■ Coccyx: Also known as the tailbone, the coccyx is the lowest part of the vertebral
column and is composed of four fused vertebrae. It is attached to the sacral
hiatus by ligaments. The prominent laminae of the first coccygeal vertebrae are
called the coccygeal cornua.
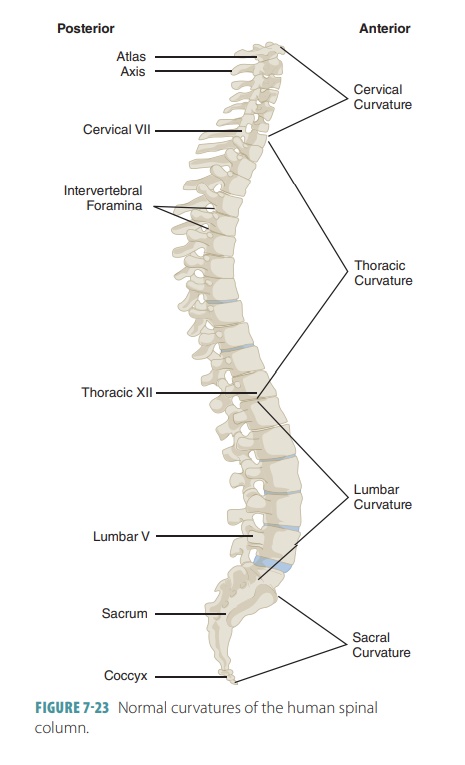
Spinal Curvature
The vertebral column consists of
four spinal curves: the cervical, thoracic, lumbar, and sacral curves. The
thoracic and sacral curves are called primary
curves. They are also called
accommoda-tion curves because they accommodate the thoracic and
abdominopelvic viscera. The cervical and lumbar curves are called secondary curves (FIGURE 7-23). They
are also called compensation curves because they help shift body
weight to allow an upright posture.
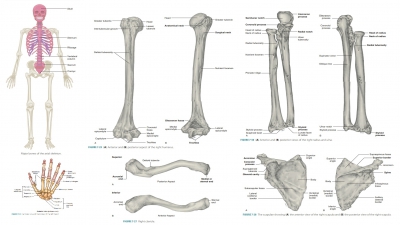
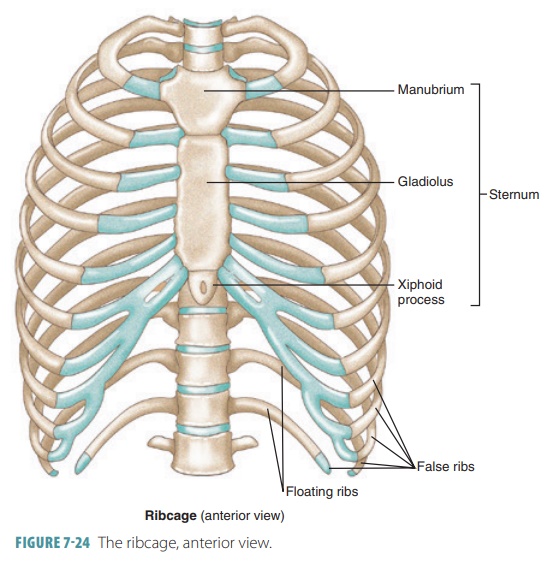
Thorax
The thorax is composed of the thoracic cage, which
includes 12 pairs of ribs connected posteriorly to the thoracic vertebrae (FIGURE 7-24), the
sternum, and the costal cartilages, which attach the ribs to the sternum
anteriorly. The thoracic cage supports the pectoral gir-dle and upper limbs and
protects the visceral organs inside the thoracic and upper abdominal cavities.
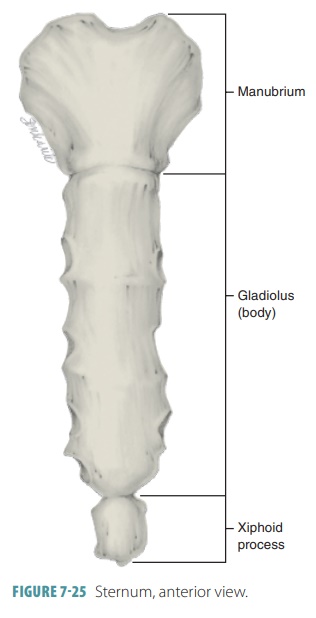
Sternum
The sternum, also known as the breastbone,
is located in the middle anterior thoracic cage. It is composed of an upper manubrium, a
middle body or gladiolus, and a lower xiphoid
process (FIGURE
7-25). The manubrium attaches to the
clavicles via clavicular
notches. It also articulates with the
first two pairs of ribs. The jugular notch is a shallow indentation between the clavicular articulations, on the
manubrium’s superior surface. It can be easily felt through the skin of the
upper chest, and is usually in line with the disc between the second and third
thoracic vertebrae as well as the point where the left common carotid artery
emerges from the aorta. The sternum is about six inches in length. Its
gladiolus is the largest portion, with notches present at the points with which
it articulates with the costal cartilages of the second to the seventh ribs.
The xiphoid process may vary in shape, and during early life is formed from
hya-line cartilage. Past the age of 40, it usually ossifies. The xiphoid
process only articulates with the gladiolus and is an attachment point for
certain abdominal muscles. In certain people, the xiphoid process projects
posteriorly, and chest trauma may plunge it
into the heart or liver, resulting in serious hemorrhaging.
Aside from the jugular notch, the
other two important anatomical landmarks of the sternum are the sternal angle and the xiphisternal joint. The sternal angle is
a horizontal ridge across the front of the sternum where the manubrium meets
the ster-nal body. It is cartilaginous, acting as a hinge to allow the
gladiolus to move anteriorly during inhala-tion. It is lined with the disc
between the fourth and fifth thoracic vertebrae, at the level of the second rib
pair. It aids in finding the second rib during physical examinations, used in
counting the ribs and a point to listen to sounds made by certain heart valves.
The xiphisternal joint is located where the gladiolus is fused with the xiphoid process. It is
located at the level of the ninth thoracic vertebra. The heart is located on
the diaphragm, just deep to the xiphisternal joint.
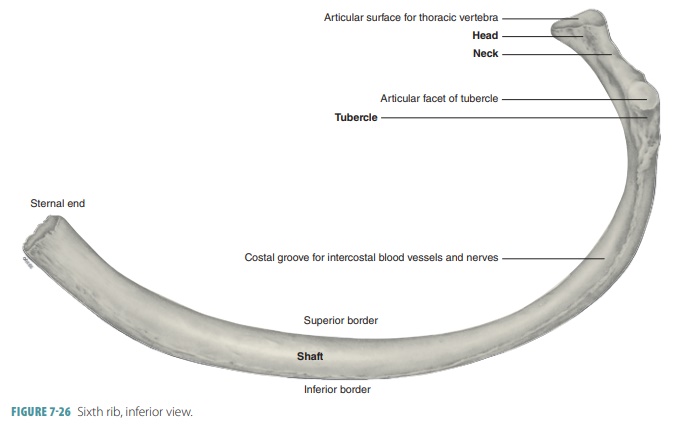
Ribs
The ribs are attached, in pairs, to each of the 12 thoracic vertebrae, totaling
24 ribs in all. The first seven pairs are true
ribs (vertebrosternal ribs), attached
to the sternum via costal cartilages.
The last five pairs are false ribs (meaning their cartilages do not reach the sternum directly). The cartilages of the upper three false rib pairs join the
cartilages of the seventh true ribs. The final two false rib pairs are called floating ribs
(vertebral ribs) because they do not attach to the sternum via cartilage. Ribs
are curved with enlarged ends (heads),
allowing them to attach to the sternum via facets (surfaces where bones meet).
The transverse process of the vertebrae articulates with a tubercle (projection) close to the rib’s head. The angle of a rib
is where the tubular shaft (body)
begins to curve toward the sternum. FIGURE 7-26 illus-trates the structure of the sixth rib in its anterior view.
1. Compare
the axial skeleton with the appendicular skeleton.
2. Explain
the bones of the cranium.
3. List
the facial bones.
4. Compare
the mandible with the hyoid bone.
1. List
the numbers of cervical, thoracic, and lumbar vertebrae.
2. Explain
the structure of the sternum.
3. Distinguish
between true, false, and floating ribs.
Related Topics