Antagonism
| Home | | Pharmacology |Chapter: Essential pharmacology : Pharmacodynamics Mechanism Of Drug Action; Receptor Pharmacology
When one drug decreases or abolishes the action of another, they are said to be antagonistic:
ANTAGONISM
When one drug decreases or abolishes the action of another, they are said to be antagonistic:
effect of drugs A + B < effect of drug A + effect of drug B
Usually in an antagonistic pair one drug is inactive as such but decreases the effect of the other. Depending on the mechanism involved, antagonism may be:
(a) Physical antagonism
Based on the physical property of the drugs, e.g. charcoal adsorbs alkaloids and can prevent their absorption—used in alkaloidal poisonings.
Radioligand binding studies have helped in characterizing and classifying receptors even when they have been dissociated from the effector system.
Many drugs act upon physiological receptors which mediate responses to transmitters, hormones, autacoids and other endogenous signal molecules; examples are cholinergic, adrenergic, histaminergic, steroid, leukotriene, insulin and other receptors. In addition, now some truly drug receptors have been described for which there are no known physiological ligands, e.g. benzodiazepine receptor, sulfonylurea receptor, cannabinoid receptor.
(b) Chemical antagonism
The two drugs react chemically and form an inactive product, e.g.
§ KMnO4 oxidizes alkaloids—used for gastric lavage in poisoning.
§ Tannins + alkaloids—insoluble alkaloidal tannate is formed.
§ Chelating agents (BAL, Cal. disod. edetate) complex toxic metals (As, Pb).
§ Nitrites form methaemoglobin which reacts with cyanide radical.
Drugs may react when mixed in the same syringe or infusion bottle:
§ Thiopentone sod. + succinylcholine chloride
§ PenicillinG sod. + succinylcholine chloride
§ Heparin + penicillin/tetracyclines/streptomycin/hydrocortisone
c) Physiological/Functional Antagonism
The two drugs act on different receptors or by different mechanisms, but have opposite overt effects on the same physiological function, i.e. have pharmacological effects in opposite direction, e.g.
• Histamine and adrenaline on bronchial muscles and BP.
• Hydrochlorothiazide and triamterene on urinary K+ excretion.
• Glucagon and insulin on blood sugar level.
(d) Receptor Antagonism
One drug (antagonist) blocks the receptor action of the other (agonist). This is a very important mechanism of drug action, because physiological signal molecules act through their receptors, blockade of which can produce specific and often profound pharmacological effects. Receptor antagonists are selective (relatively), i.e. an anticholinergic will oppose contraction of intestinal smooth muscle induced by cholinergic agonists, but not that induced by histamine or 5HT (they act through a different set of receptors). Receptor antagonism can be competitive or noncompetitive.
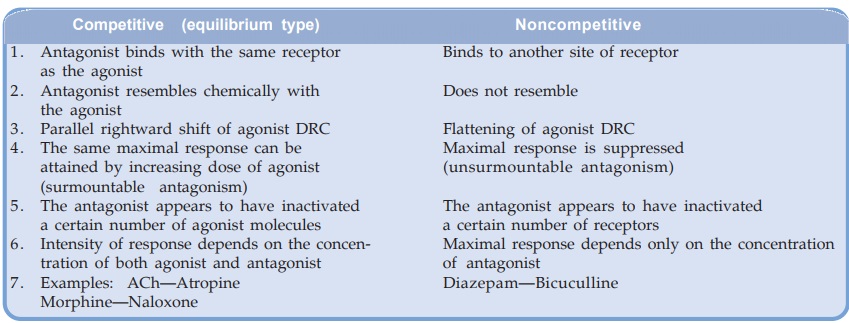
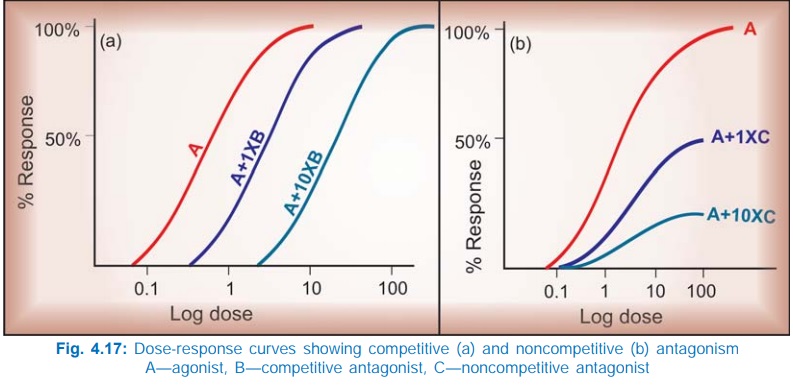
Competitive antagonism (equilibrium type) The antagonist is chemically similar to the agonist, competes with it (Fig. 4.16 A, D) and binds to the same site to the exclusion of the agonist molecules. Because the antagonist has affinity but no intrinsic activity (see p. 42), no response is produced and the log DRC of the agonist is shifted to the right. Since antagonist binding is reversible and depends on the relative concentration of the agonist and antagonist molecules, higher concentration of the agonist progressively overcomes the block—a parallel shift of the agonist DRC with no suppression of maximal response is obtained (Fig. 4.17a). The extent of shift is dependent on the affinity and concentration of the antagonist.
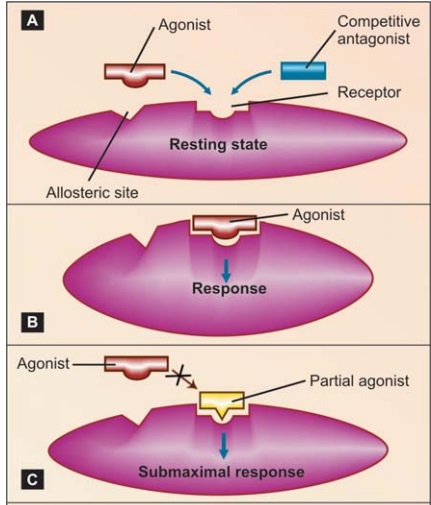
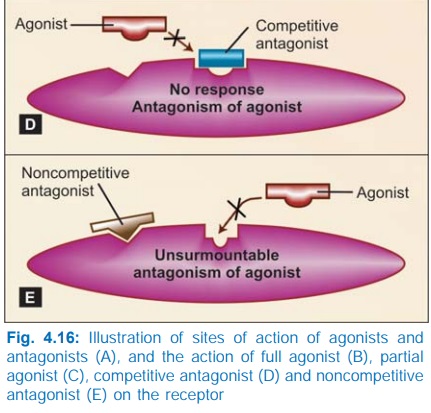
A partial agonist (Fig. 4.16 C), having affinity for the same receptor, also competes with and antagonizes a full agonist, while producing a submaximal response of its own.
Noncompetitive antagonism The antagonist is chemically unrelated to the agonist, binds to a different allosteric site altering the receptor in such a way that it is unable to combine with the agonist (Fig. 4.16E), or unable to transduce the response, so that the downstream chain of events are uncoupled. Because the agonist and the antagonist are combining with different sites, there is no competition between them—even high agonist concentration is unable to reverse the block completely. Increasing concentrations of the antagonist progressively flatten the agonist DRC (Fig. 4.17b). Noncompetitive antagonists have been produced experimentally, but are not in clinical use.
Nonequilibrium (competitive) antagonism Certain antagonists bind to the receptor with strong (covalent) bonds or dissociate from it slowly so that agonist molecules are unable to reduce receptor occupancy of the antagonist molecules— law of mass action cannot apply—an irreversible or nonequilibrium antagonism is produced. The agonist DRC is shifted to the right and the maximal response is lowered (if spare receptors are few). Since flattening of agonist DRC is a feature of noncompetitive antagonism; nonequilibrium antagonism has also been called ‘a type of noncompetitive antagonism’. This appears inappropriate because the antagonist is binding to the same site as the agonist. Phenoxybenzamine is a nonequilibrium antagonist of adrenaline at the α adrenergic receptors.
Features of competitive and noncompetitive antagonism are compared below: